Dear Agent,
STILLWATER (145,000 words) is a character-driven, modern retelling of Jane Austen’s most controversial novel, Mansfield Park. Set in a historic plantation house in the sugarlands of Louisiana, this novel will appeal to readers searching for reimaginings of Austen such as Miss Austen by Gill Hornby, or Whit Stillman’s novel Love and Friendship. Even without reference to Austen, STILLWATER can be appreciated in its own right as literary fiction in the style of A Gentleman in Moscow by Amor Towles.
Stillwater, owned by the Andrews family since before the Civil War, is the grandest surviving plantation house in Louisiana, and petite Cajun Melly Arceneaux its humblest resident. Painfully introverted, physically fragile, informally adopted by her benignly neglectful Andrews godparents, Melly prefers to linger in the shadows of her beloved Stillwater as a companion and drudge. As long as she can depend on the friendship of idealistic seminarian turned teacher Malcolm Andrews, and escape the notice of his worldly siblings and the ruthlessly efficient estate manager Esther Davis, she is content.
But when a pair of dazzlingly amoral siblings from New York City, Alys and Ian Winter, take a lease on one of Stillwater's old cottages, Melly finds her friendship with Malcolm, her secure home, and her integrity assailed from every side. The Winters, cheerfully ready to disrupt every aspect of life at Stillwater, discover to their fascination that Melly’s meekness can hide an astonishing reserve of fierce inner strength. And Melly will discover whether she has the courage not only to stand alone in her convictions, but to fight for Malcolm and for Stillwater at the risk of losing them forever.
I live in Ohio, and grew up making summer visits to my grandparents in their antebellum home near Baton Rouge. Theater is my first love, but reading classic literature aloud to my children is a close second.
Thank you for considering my novel, and I look forward to hearing from you.
Sincerely,
MrsDarwin
Saturday, May 23, 2020
Thursday, May 21, 2020
Understanding the COVID-19 Outbreak: Part 4
This is the fourth installment of this increasingly long series on the COVID-19 pandemic. You can read Part 1, Part 2, and Part 3 at these links. In this post, I'll assess the outbreak by the numbers and try to address the question of whether by those numbers the coronavirus can rightly be called a pandemic at all.
The Numbers
Various other commitments have slowed me down over the last few days, but I want to turn now to the question of numbers. As I discussed in Part 3, the definition of a pandemic is a disease that affects a large number of people throughout the world. One of the difficulties in assessing events as they happen is that we often know less about the present than we do about the past. With the past, we have the benefit of knowing where things are going, how the story ends, and we also have the time to gather information from many sources, the time to organize information and sift it. The coronavirus pandemic has been a blogger's and even more so a Tweeter's kind of news story. There are multiple online data sources which are posting data in what seems like nearly live time. You can go to the John Hopkinds University dashboard or the Worldometers coronavirus webpage or the Covid Tracking Project and see new statistics appearing every few minutes. The CDC and many states, counties, and even cities have set up their own data dashboards where they publish daily data. People representing important institutions have gone on TV and announced that they have built statistical models which can predict what will happen if various actions are taken and how the outbreak will progress. All of this gives an appearance of a situation where we know a great deal and can make the predictions with all the authority of techs crouched over computer screens and plotting the trajectory of a space capsule.
And yet, think for a moment about where all this seemingly abundant data comes from.
A disease is not a web stat or a stock market price or some other thing which is collected directly into a computer at the moment it happens. Someone gets sick. Maybe they take a test. Maybe they don't. If they do take a test, some amount of data may be collected about them: when did they get sick, how old are they, where have they been, who have they been near. Or it may not. That data may be collected to some central repository in a useful way, or it may not.
Someone dies. That person has been sick. Was it coronavirus? Was the person tested? How sick were they before? How old were they. When and where did they even die?
When people are massively overwhelmed with the difficulty of fighting a serious disease outbreak, they may get messier about collecting data. If they have almost no infections of a particular disease in the area, they may not think to test for it. Or they may try to test, but not have a good way to report the results.
The result of all this is that although we receive new data constantly, the data we have is at best a partial view of what is really going on out in the world, and the relationship between this partial view and the world itself is a matter of some dispute. Combine this with people who have decided to address the facts ideologically or who are determined to either minimize or maximize the pandemic in order to alleviate their particular emotional reactions to it, and there is a great deal of confusion out there.
I'll run through the basic numbers and to what extent we do or do not know them.
The number of people who now have or have in the past been infected by the SARS-CoV-2 virus: This number is hard to know with any certainty right now, because not all people who are sick are tested, sometimes the test provides a false negative result, and many people (though what percentage we don't know) are infected by the virus and are contagious but don't show any symptoms. Probably at some point in the future epidemiologists will have some sort of a backward looking estimate of the number, but even that will be based on assumptions we can't totally prove. This is no different from any other major disease. We do not, for instance, know with any great certainty how many people had the 1918 Spanish Flu, or how many people had AIDS or Ebola, etc.
The number of people who have tested positive for actively having COVID-19 (the disease caused by the virus SARS-CoV-2): This number is clearly reported and you can download the data from many sources. The only thing that is a little bit confusing is knowing when the person who tested positive first got the virus. There can be a lag of some days or even a couple weeks between when someone gets the virus and when they are tested and get a positive result. This means that the number of positive tests that are recorded on a given day can be a mix of people who contracted the virus up to a few weeks before and people who got it quite recently.
The number of people who have ever had the virus: This can be estimated with antibody tests, tests that analyze someone's blood and look for the antibodies that the body makes to fight off the SARS-CoV-2 virus. If someone has those antibodies, we can conclude that that person at some point contracted the virus. There have been a number of tests of this type conducted in different regions and with different sampling techniques. They have so far produced widely varying estimates of how many people have had the virus in different parts of the country. I think in the long run, major well run studies will establish this pretty clearly, but right now there are a lot of flaky, tiny studies out there, some of which are being run by people with agendas or with very poor methodologies.
The number of people who are hospitalized as a result of the virus: This number we know moderately well, so long as enough tests are available to test people who are under care because of symptoms which appear to be similar to the virus. However, here we run into reporting issues: not all hospitals have the time and resources to report on how many COVID-19 patients they have consistently, and not all cities and states are collecting and tabulating the data in the same way. This is something that in the long run will probably be known pretty well but which right now can be tricky to sort out clearly.
The number of people who have died as a result of the virus: You would think it would be pretty easy to know if people had died or not. Overall, I think number of deaths due to COVID-19 is probably one of the clearer measures that we have right now. However, even here we have the difficulty of diagnosis. If someone died after having been sick with symptoms that look like COVID-19, but that person has not been tested, whether they are classified as being a COVID-19 death will depend on the reporting agency tabulating the results. Some countries are also overwhelmed or do not have very good data gathering systems, and so their tabulations of deaths are simply not good. A few countries don't even keep accurate records of how many people die. And even in the US, although we have pretty meticulous data on deaths, our systems got gathering it are slow, as cities report to states and states report to the CDC. As a result, although through one system we have people reporting to the CDC very quickly how many people are dying of COVID-19, our data on how many people have died in total is partial for up to a couple months until all the data gathering and cleaning is done.
The percent of people who get the virus who die as a result: This number is trickier to get than you would think. Say you pull up a dashboard right at this moment and you see that the US has 1,573,073 cases of COVID-19 to date and 93,653 deaths. Simple division would tell you that 6% of cases result in death. This is called the Case Fatality Rate or CFR, and you'll hear that number thrown around. But as I discussed above, although we know how many people have tested positive for the coronavirus, we don't know how many people have actually had it. We can be pretty sure that we haven't tested very person who is sick. So the denominator of that fatality rate equation if we wanted to calculate the actual changes of someone dying due to the virus is some number bigger than 1.5 million. But how much bigger? If the number of people who have actually had the virus is five times larger, then the fatality rate is 1.2%. If it's ten times larger, then the fatality rate is 0.6%. If we've only tested 1 out of a hundred of the people who are actually sick, then the fatality rate is only 0.1% and is similar to the seasonal flu. But if we were to assume that the number of people actually sick is 100x the number of positive tests, we'd have to say that 157 million people have had the virus, almost half the US population. That seems very, very hard to believe, and it doesn't align with any of the serology tests I mentioned above. FFor instance, an antibody test in New York in late April found that about 25% of people in New York City (the area hit by far the hardest) had had the virus. Given the number of deaths New York City had experienced at the time, that would suggest an average fatality rate of around 0.5% or about 5x the fatality rate of the seasonal flu. (The Santa Clara study that the linked article also mentions has been widely questioned and should probably be ignored because most of the positive may have been false positives.)
All of this should make clear, there are a lot of things that we don't know when it comes to the numbers that surround the pandemic. What basic things can we draw from the available data? What things can we conclude are definitely not true?
We know that it is a serious disease which is capable of spreading through a significant percentage of the population and causing a large number of deaths. And we know that these deaths are not just expected deaths from flu or pneumonia that are being mis-categorized. Let's look at some New York data to validate this.
The first look is simple. Pulling data from the COVID-19 Project, I built a basic chart of New York State reported COVID-19 deaths by day with a 7-day moving average:
 This seems pretty straight forward. It increases sharply near the beginning. Then it peaks and it goes down more slowly. There are a total of almost 23,000 deaths. And yet, some might ask, how do we know these are actually unexpected deaths? Lots of people die every day. Indeed, in the long run, 100% of people die. So how do we know these deaths aren't just like a "bad flu season" but being blown out of proportion by media frenzy and political passions? We can examine that question a bit on our own. The CDC has a data repository that allows us to look at weekly deaths due to flu, pneumonia, and total deaths by week either nationally or by state/region. I've downloaded the data for New York State. Here's data for total deaths and for flu/pneumonia since mid 2015:
This seems pretty straight forward. It increases sharply near the beginning. Then it peaks and it goes down more slowly. There are a total of almost 23,000 deaths. And yet, some might ask, how do we know these are actually unexpected deaths? Lots of people die every day. Indeed, in the long run, 100% of people die. So how do we know these deaths aren't just like a "bad flu season" but being blown out of proportion by media frenzy and political passions? We can examine that question a bit on our own. The CDC has a data repository that allows us to look at weekly deaths due to flu, pneumonia, and total deaths by week either nationally or by state/region. I've downloaded the data for New York State. Here's data for total deaths and for flu/pneumonia since mid 2015:
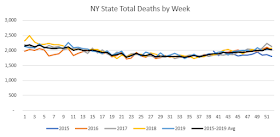
 As you can see, the trends are fairly predictable. 2016 was a pretty mild flu year. 2018 was a fairly bad one. But the lowest variance I see of any week's total deaths below the average is Week 6 (mid Feb) in 2016 which was 263 deaths below the average of 2,077. The highest variance was in Week 2 of 2018 when total deaths were 298 above the average of 2,195. Thus, each year's actual total deaths by week are within +/- 15% of the average.
As you can see, the trends are fairly predictable. 2016 was a pretty mild flu year. 2018 was a fairly bad one. But the lowest variance I see of any week's total deaths below the average is Week 6 (mid Feb) in 2016 which was 263 deaths below the average of 2,077. The highest variance was in Week 2 of 2018 when total deaths were 298 above the average of 2,195. Thus, each year's actual total deaths by week are within +/- 15% of the average.
Now let's look at this year.
 Whereas the most variation we'd seen before was 15%, here we have two weeks that are more than 100% above the average. If I sum the total "excess deaths" (the space between the orange line representing this year and the black line representing the average) we get 8,251 deaths. That's actually significantly less than the reported New York State deaths to date, but the most recent weeks of this CDC death data are incomplete, and it doesn't even have weeks 20-21. As the year progresses, we'll able to see how this settles out, and we'll also see whether we see lower than average deaths through the rest of the year, which would support the claim some have made that many of these people would have died soon anyway. (I do not expect that's what we'll find.)
Whereas the most variation we'd seen before was 15%, here we have two weeks that are more than 100% above the average. If I sum the total "excess deaths" (the space between the orange line representing this year and the black line representing the average) we get 8,251 deaths. That's actually significantly less than the reported New York State deaths to date, but the most recent weeks of this CDC death data are incomplete, and it doesn't even have weeks 20-21. As the year progresses, we'll able to see how this settles out, and we'll also see whether we see lower than average deaths through the rest of the year, which would support the claim some have made that many of these people would have died soon anyway. (I do not expect that's what we'll find.)
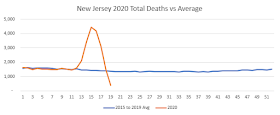
We see the same thing with other states we've been hearing about in the news. In New Jersey there are 10,147 excess deaths in the data thus far, with the top week 208% above the average.
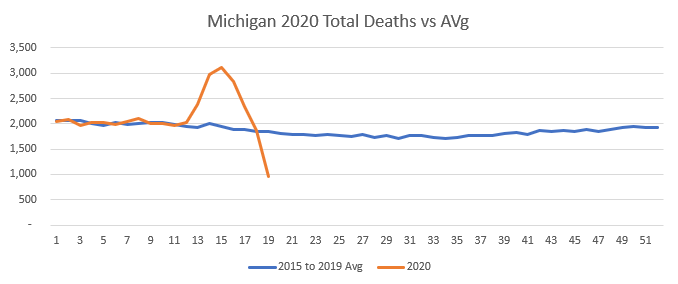
 In Michigan, 3,985 excess deaths thus far, with the top week 59% above the average.
In Michigan, 3,985 excess deaths thus far, with the top week 59% above the average.
 These spikes in deaths are far, far outside anything that we've seen due to season flu. In New York State, the worst spike above average in the last five years was 298 deaths in Week 2 of 2018. Here we're seeing an effect which is more than seven times bigger than that. Indeed, the excess NY State deaths in April of 2020 look like they'll be at least 2x the number of excess deaths in September 2001.
These spikes in deaths are far, far outside anything that we've seen due to season flu. In New York State, the worst spike above average in the last five years was 298 deaths in Week 2 of 2018. Here we're seeing an effect which is more than seven times bigger than that. Indeed, the excess NY State deaths in April of 2020 look like they'll be at least 2x the number of excess deaths in September 2001.
So far, the coronavirus is an intensely regional problem. Some states have very bad outbreaks and some have very mild ones. Yet even so, the impact is measurable on a national level even though data is still far from complete for the last couple months.
 I've done a couple things with this graph to try to make it readily understandable. (Click on it to get a larger image.) I've made the multi-year average a heavy black line, and this year is a heavy red line. Other years are in colors and are much thinner lines. However, I've made 2018 a medium thickness orange line, because the 2017-2018 flu season is an example of a particularly bad recent flu season. If I compare late 2017 and early 2018 to the national average, I come up with around 38,000 excess deaths from that flu season, with the worst weeks being 10% above the average. With the COVID-19 outbreak in 2020, I'm showing 50,000 excess deaths with the worst week being 30% above average. However, let me emphasize, the most recent weeks do not have complete data. You can see that with the way that the red line falls off the bottom of the graph in Week 19. That's not because no one died. It's because the CDC doesn't have complete data. It will continue to revise the most recent 10-13 rolling weeks as it moves forward, so we won't have a fully clear view of this April/May time period until August or September. (I fully intend to check back and provide more analysis at that point.)
I've done a couple things with this graph to try to make it readily understandable. (Click on it to get a larger image.) I've made the multi-year average a heavy black line, and this year is a heavy red line. Other years are in colors and are much thinner lines. However, I've made 2018 a medium thickness orange line, because the 2017-2018 flu season is an example of a particularly bad recent flu season. If I compare late 2017 and early 2018 to the national average, I come up with around 38,000 excess deaths from that flu season, with the worst weeks being 10% above the average. With the COVID-19 outbreak in 2020, I'm showing 50,000 excess deaths with the worst week being 30% above average. However, let me emphasize, the most recent weeks do not have complete data. You can see that with the way that the red line falls off the bottom of the graph in Week 19. That's not because no one died. It's because the CDC doesn't have complete data. It will continue to revise the most recent 10-13 rolling weeks as it moves forward, so we won't have a fully clear view of this April/May time period until August or September. (I fully intend to check back and provide more analysis at that point.)
Even so, you might ask yourself: Why are we shutting the country down? We did basically nothing to stop the 2017-2018 flu season, and we just accepted those "excess deaths" which are themselves in excess of season flu deaths that we suffer every year without shutting the economy down. So why are we doing this now? Is there something acceptable about 38,000 excess deaths that's totally unacceptable about 50,000?
The answer lies in the question. There's been an unprecedented effort to reduce the chances for this virus to spread since we as a country got serious about things in the middle of March. Apple provides a really interesting tool which allows you to see how much people's use of their Maps app to travel had gone down in various areas. Take a look:
 All that reduction in moving around represents people going fewer places and spending less time around other people. And if we think back to the question of how a virus spreads, it's all a mathematical function of how easily it is spread from one person to another, and how many other people a sick person comes in contact with. If you have a one in 50 chance of passing the virus to each person you interact with during a two week period of being contagious, then it matters a lot whether you come in contact with 10 people or 200 people during that two week period.
All that reduction in moving around represents people going fewer places and spending less time around other people. And if we think back to the question of how a virus spreads, it's all a mathematical function of how easily it is spread from one person to another, and how many other people a sick person comes in contact with. If you have a one in 50 chance of passing the virus to each person you interact with during a two week period of being contagious, then it matters a lot whether you come in contact with 10 people or 200 people during that two week period.
Having spent so much time discussing the virus online over the last few weeks, I can already hear someone saying, "What about Sweden? They haven't shut down, and they're doing okay." Well, okay is relative. They're hit much harder than the other Scandinavian countries in terms of deaths so far. But more importantly, just because they haven't had a legal "lockdown" doesn't mean that they aren't circulating a lot less. Here's the same movement graph for Sweden.
 So Swedes actually are staying home a lot more, and in particular they're using public transit 33% less than they were before. And as a result, their economy is seeing a lot of the same slowdown that we are.
So Swedes actually are staying home a lot more, and in particular they're using public transit 33% less than they were before. And as a result, their economy is seeing a lot of the same slowdown that we are.
So while it's true that so far (and there's a lot of emphasis in that "so far" because our data isn't nearly complete yet) the number of excess deaths we can measure is less than twice that of a bad though normal flu season, that's within the context of an outbreak which we've put the brakes on by having everyone hunker down. And even as people now begin to return to more normal activities, they're doing so with a much greater than normal awareness of avoiding behavior that might pass on a respiratory virus. In that sense, it would seem likely that the virus is spreading significantly more slowly now than in a "do nothing" scenario such as our normal response to flu season. If we were going to try to say whether our response to the risk of the virus was proportional to the danger we faced, we need to look not at what's actually happened (which is 90,000 deaths according to the official tally and 50,000 according to the far-from-complete "excess death" analysis) but rather try to get some sense of what could have happened if we had not acted to drastically slow the spread of the virus.
Let's try a basic range of assumptions that seem within the realm of possibility. We know that there are 330,000,000 people in the US. Say that the ~25% infection rate for New York City which is suggested by antibody tests is actually the outer bound of how many infections a region could have before it peters out due to not having enough non-immune hosts left available. (For comparison, estimates are that it was about 25% of the US population that got Spanish Flu back in 1918 as well.) And say that the 0.5% infection fatality rate that suggests given New York City's death numbers is also correct. 330M times 25% times 0.5% is 412,000 deaths. Let's take that as our low number. For a mid number, let's assume that NYC is actually not at the maximum saturation point for infections. Maybe if we pretty much went about our normal lives about 40% of the population would get the virus. If we assume 40% infections and 0.5% mortality, we get 660,000 deaths. For our worst case scenario, let's imagine a 40% infection rate but also that the fatality rate that I'm estimating is a bit low. What if it's more like 1%, which I think is about the upper bound of the reasonable infection fatality rates that I've seen. Those assumptions get us to 1,320,000 deaths.
So if we hadn't done all this to try to stop the spread of the virus, there's a pretty decent possibility that we would be facing 400k to 1.3M deaths. I think we could all agree that's a really large number, and one it would be reasonable to take some pretty drastic actions to avoid. If the actions we're taking can reduce those down to something in the 100k to 200k range, it seems like that would be a potentially reasonable course of action. (I want to examine in depth the question of whether "lockdowns" actually save lives or just space them out over more time, but I think that needs its own post.)
However, a counter-argument that is often made is that while COVID-19 causes a lot of deaths, those are actually deaths that would have occurred soon anyway. According to this argument, the virus is mostly killing people who are very old and/or have existing conditions that put them in fragile health.
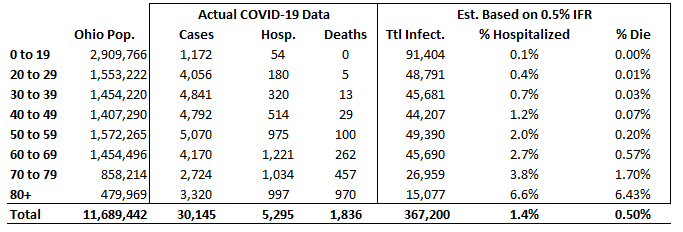
This is to some extent true. Here's a shot of the COVID-19 dashboard for my state of Ohio. I think it does a really good job of showing the dynamics of the virus:
 Note that while actual cases are spread pretty evenly across the whole population, with the exception of kids, more than half of the 1,836 deaths were among people who were 80+.
Note that while actual cases are spread pretty evenly across the whole population, with the exception of kids, more than half of the 1,836 deaths were among people who were 80+.
So what does this mean in terms of the actual chance that people with COVID-19 will end up in the hospital or will end up dead? As we discussed earlier, lots of people who have the virus have not actually been tested, so the case numbers don't tell us everything. I also said that 0.5% overall fatality rate for all infections (not just identified cases) seems like a pretty plausible number based on the antibody studies from New York City. So here I've taken the Ohio population, assumed that actual infections are evenly distributed across the population even though the very mild nature of the disease in younger people means that fewer cases have been identified among the younger age groups, and projected an estimated total number of infections based on a total population IFR of 0.5%. (In other words, I first calculated that there were 367,200 infections by assuming that the 1,836 deaths represented a 0.5% IFR, and then spread those infections across the age groups based on the percent of Ohio residents in each age group.)
 Having done that, I calculated what the hospitalization rate was for each age group. The answer? For people who are 80%, 6.4% of estimated infections were fatal. For people in their 20s, only 0.01% were fatal. Hospitalization rates are a bit higher. There's a 1.2% chance for someone in their 40s who gets the virus having a bad enough case to end up in the hospital. But the rates are still overall low. Indeed, so low that you may be thinking: Why worry? This looks like nothing!
Having done that, I calculated what the hospitalization rate was for each age group. The answer? For people who are 80%, 6.4% of estimated infections were fatal. For people in their 20s, only 0.01% were fatal. Hospitalization rates are a bit higher. There's a 1.2% chance for someone in their 40s who gets the virus having a bad enough case to end up in the hospital. But the rates are still overall low. Indeed, so low that you may be thinking: Why worry? This looks like nothing!
Well, for a lot of people the virus does give no symptoms at all or very mild symptoms. But keep in mind, we have a lot of people in our country. There are 12.5M people over 80 in the US. Apply these rates across the whole US population and you get to some large numbers. Let's go back to our minimum scenario where 25% of the US population got the virus. What would these hospitalization rates and fatality rates mean in terms of total deaths for different age groups? What I've done here is calculated 25% of the US population as the total number of infections and then distributed those infections evenly across the population according to how many people are in each age group. Obviously, there are a lot of assumptions being made here, but as a conservative scenario I don't think it's unreasonable.
 How do we think about this? 400,000 Americans dead is a lot of people. Three quarters of them would be seventy or over, but there are plenty of people who are seventy years old who have ten or twenty good years of life before them. Does this call for the kind of massive actions that we've taken or not? How do we think about the 10% of Americans who would be suffering 75% of the deaths? I'm not going to say that that's a super easy question. And of course, these are only rough estimates made based on multiple assumptions. We had less data when we were making the decisions that put us into this position back in March -- though we did have a fair amount of the data. I want to dig more deeply into the question of the "lockdowns" in the next post, but before I do that I'd like to point out that we often get too locked into talking about deaths only. Death is coming for all of us, and yet we don't want to die early, nor do we want to see our loved ones do so.
How do we think about this? 400,000 Americans dead is a lot of people. Three quarters of them would be seventy or over, but there are plenty of people who are seventy years old who have ten or twenty good years of life before them. Does this call for the kind of massive actions that we've taken or not? How do we think about the 10% of Americans who would be suffering 75% of the deaths? I'm not going to say that that's a super easy question. And of course, these are only rough estimates made based on multiple assumptions. We had less data when we were making the decisions that put us into this position back in March -- though we did have a fair amount of the data. I want to dig more deeply into the question of the "lockdowns" in the next post, but before I do that I'd like to point out that we often get too locked into talking about deaths only. Death is coming for all of us, and yet we don't want to die early, nor do we want to see our loved ones do so.
But as we think about how much people would want to avoid getting this disease, how much they would stay away from restaurants and big gatherings in order to stay healthy even if not ordered to, and slow down the consumer economy as they did so, it's worth looking at the other set of estimates. Someone in his forties is almost a hundred times less likely to die if infected with the virus as someone who is 80+, but he's still a sixth as likely to end up in the hospital. While my estimate is that if 25% of Americans got the coronavirus, only 90,000 people under 70 would die of it, over 700,000 people under 70 would spend time in the hospital. Indeed, while 75% of the deaths would be people over 70, more than 60% the people hospitalized would be people under 70. 20% of the people hospitalized would be under fifty. 10% of people hospitalized would be under forty. I think we have to assume that there would be lots of other people who never ended up in hospitals but who felt really, really sick and scared for a couple weeks as they waited to see if they'd end up having to go to the hospital.
There are a lot of things that we don't know about this virus, and there are a lot of things we can reasonably argue about in how to respond to it. However, I think that this examination of the numbers underlines that while there have definitely been panicked numbers thrown around by people who didn't know what they were doing (I don't think that claims we'd see 5-10 million deaths ever fit well with what we knew, even back in February) this is a serious disease which, if left unchecked, could be responsible for a lot of deaths and a great deal of suffering. Hopefully this provides some insight into just what the dimensions of those possibilities are (and aren't.)
In my next post, I'll talk about the measures that have been taken to suppress the virus, including the "lockdowns" which are the subject of so much political dispute.
The Numbers
Various other commitments have slowed me down over the last few days, but I want to turn now to the question of numbers. As I discussed in Part 3, the definition of a pandemic is a disease that affects a large number of people throughout the world. One of the difficulties in assessing events as they happen is that we often know less about the present than we do about the past. With the past, we have the benefit of knowing where things are going, how the story ends, and we also have the time to gather information from many sources, the time to organize information and sift it. The coronavirus pandemic has been a blogger's and even more so a Tweeter's kind of news story. There are multiple online data sources which are posting data in what seems like nearly live time. You can go to the John Hopkinds University dashboard or the Worldometers coronavirus webpage or the Covid Tracking Project and see new statistics appearing every few minutes. The CDC and many states, counties, and even cities have set up their own data dashboards where they publish daily data. People representing important institutions have gone on TV and announced that they have built statistical models which can predict what will happen if various actions are taken and how the outbreak will progress. All of this gives an appearance of a situation where we know a great deal and can make the predictions with all the authority of techs crouched over computer screens and plotting the trajectory of a space capsule.
And yet, think for a moment about where all this seemingly abundant data comes from.
A disease is not a web stat or a stock market price or some other thing which is collected directly into a computer at the moment it happens. Someone gets sick. Maybe they take a test. Maybe they don't. If they do take a test, some amount of data may be collected about them: when did they get sick, how old are they, where have they been, who have they been near. Or it may not. That data may be collected to some central repository in a useful way, or it may not.
Someone dies. That person has been sick. Was it coronavirus? Was the person tested? How sick were they before? How old were they. When and where did they even die?
When people are massively overwhelmed with the difficulty of fighting a serious disease outbreak, they may get messier about collecting data. If they have almost no infections of a particular disease in the area, they may not think to test for it. Or they may try to test, but not have a good way to report the results.
The result of all this is that although we receive new data constantly, the data we have is at best a partial view of what is really going on out in the world, and the relationship between this partial view and the world itself is a matter of some dispute. Combine this with people who have decided to address the facts ideologically or who are determined to either minimize or maximize the pandemic in order to alleviate their particular emotional reactions to it, and there is a great deal of confusion out there.
I'll run through the basic numbers and to what extent we do or do not know them.
The number of people who now have or have in the past been infected by the SARS-CoV-2 virus: This number is hard to know with any certainty right now, because not all people who are sick are tested, sometimes the test provides a false negative result, and many people (though what percentage we don't know) are infected by the virus and are contagious but don't show any symptoms. Probably at some point in the future epidemiologists will have some sort of a backward looking estimate of the number, but even that will be based on assumptions we can't totally prove. This is no different from any other major disease. We do not, for instance, know with any great certainty how many people had the 1918 Spanish Flu, or how many people had AIDS or Ebola, etc.
The number of people who have tested positive for actively having COVID-19 (the disease caused by the virus SARS-CoV-2): This number is clearly reported and you can download the data from many sources. The only thing that is a little bit confusing is knowing when the person who tested positive first got the virus. There can be a lag of some days or even a couple weeks between when someone gets the virus and when they are tested and get a positive result. This means that the number of positive tests that are recorded on a given day can be a mix of people who contracted the virus up to a few weeks before and people who got it quite recently.
The number of people who have ever had the virus: This can be estimated with antibody tests, tests that analyze someone's blood and look for the antibodies that the body makes to fight off the SARS-CoV-2 virus. If someone has those antibodies, we can conclude that that person at some point contracted the virus. There have been a number of tests of this type conducted in different regions and with different sampling techniques. They have so far produced widely varying estimates of how many people have had the virus in different parts of the country. I think in the long run, major well run studies will establish this pretty clearly, but right now there are a lot of flaky, tiny studies out there, some of which are being run by people with agendas or with very poor methodologies.
The number of people who are hospitalized as a result of the virus: This number we know moderately well, so long as enough tests are available to test people who are under care because of symptoms which appear to be similar to the virus. However, here we run into reporting issues: not all hospitals have the time and resources to report on how many COVID-19 patients they have consistently, and not all cities and states are collecting and tabulating the data in the same way. This is something that in the long run will probably be known pretty well but which right now can be tricky to sort out clearly.
The number of people who have died as a result of the virus: You would think it would be pretty easy to know if people had died or not. Overall, I think number of deaths due to COVID-19 is probably one of the clearer measures that we have right now. However, even here we have the difficulty of diagnosis. If someone died after having been sick with symptoms that look like COVID-19, but that person has not been tested, whether they are classified as being a COVID-19 death will depend on the reporting agency tabulating the results. Some countries are also overwhelmed or do not have very good data gathering systems, and so their tabulations of deaths are simply not good. A few countries don't even keep accurate records of how many people die. And even in the US, although we have pretty meticulous data on deaths, our systems got gathering it are slow, as cities report to states and states report to the CDC. As a result, although through one system we have people reporting to the CDC very quickly how many people are dying of COVID-19, our data on how many people have died in total is partial for up to a couple months until all the data gathering and cleaning is done.
The percent of people who get the virus who die as a result: This number is trickier to get than you would think. Say you pull up a dashboard right at this moment and you see that the US has 1,573,073 cases of COVID-19 to date and 93,653 deaths. Simple division would tell you that 6% of cases result in death. This is called the Case Fatality Rate or CFR, and you'll hear that number thrown around. But as I discussed above, although we know how many people have tested positive for the coronavirus, we don't know how many people have actually had it. We can be pretty sure that we haven't tested very person who is sick. So the denominator of that fatality rate equation if we wanted to calculate the actual changes of someone dying due to the virus is some number bigger than 1.5 million. But how much bigger? If the number of people who have actually had the virus is five times larger, then the fatality rate is 1.2%. If it's ten times larger, then the fatality rate is 0.6%. If we've only tested 1 out of a hundred of the people who are actually sick, then the fatality rate is only 0.1% and is similar to the seasonal flu. But if we were to assume that the number of people actually sick is 100x the number of positive tests, we'd have to say that 157 million people have had the virus, almost half the US population. That seems very, very hard to believe, and it doesn't align with any of the serology tests I mentioned above. FFor instance, an antibody test in New York in late April found that about 25% of people in New York City (the area hit by far the hardest) had had the virus. Given the number of deaths New York City had experienced at the time, that would suggest an average fatality rate of around 0.5% or about 5x the fatality rate of the seasonal flu. (The Santa Clara study that the linked article also mentions has been widely questioned and should probably be ignored because most of the positive may have been false positives.)
All of this should make clear, there are a lot of things that we don't know when it comes to the numbers that surround the pandemic. What basic things can we draw from the available data? What things can we conclude are definitely not true?
We know that it is a serious disease which is capable of spreading through a significant percentage of the population and causing a large number of deaths. And we know that these deaths are not just expected deaths from flu or pneumonia that are being mis-categorized. Let's look at some New York data to validate this.
The first look is simple. Pulling data from the COVID-19 Project, I built a basic chart of New York State reported COVID-19 deaths by day with a 7-day moving average:



Now let's look at this year.

We see the same thing with other states we've been hearing about in the news. In New Jersey there are 10,147 excess deaths in the data thus far, with the top week 208% above the average.

So far, the coronavirus is an intensely regional problem. Some states have very bad outbreaks and some have very mild ones. Yet even so, the impact is measurable on a national level even though data is still far from complete for the last couple months.

Even so, you might ask yourself: Why are we shutting the country down? We did basically nothing to stop the 2017-2018 flu season, and we just accepted those "excess deaths" which are themselves in excess of season flu deaths that we suffer every year without shutting the economy down. So why are we doing this now? Is there something acceptable about 38,000 excess deaths that's totally unacceptable about 50,000?
The answer lies in the question. There's been an unprecedented effort to reduce the chances for this virus to spread since we as a country got serious about things in the middle of March. Apple provides a really interesting tool which allows you to see how much people's use of their Maps app to travel had gone down in various areas. Take a look:

Having spent so much time discussing the virus online over the last few weeks, I can already hear someone saying, "What about Sweden? They haven't shut down, and they're doing okay." Well, okay is relative. They're hit much harder than the other Scandinavian countries in terms of deaths so far. But more importantly, just because they haven't had a legal "lockdown" doesn't mean that they aren't circulating a lot less. Here's the same movement graph for Sweden.

So while it's true that so far (and there's a lot of emphasis in that "so far" because our data isn't nearly complete yet) the number of excess deaths we can measure is less than twice that of a bad though normal flu season, that's within the context of an outbreak which we've put the brakes on by having everyone hunker down. And even as people now begin to return to more normal activities, they're doing so with a much greater than normal awareness of avoiding behavior that might pass on a respiratory virus. In that sense, it would seem likely that the virus is spreading significantly more slowly now than in a "do nothing" scenario such as our normal response to flu season. If we were going to try to say whether our response to the risk of the virus was proportional to the danger we faced, we need to look not at what's actually happened (which is 90,000 deaths according to the official tally and 50,000 according to the far-from-complete "excess death" analysis) but rather try to get some sense of what could have happened if we had not acted to drastically slow the spread of the virus.
Let's try a basic range of assumptions that seem within the realm of possibility. We know that there are 330,000,000 people in the US. Say that the ~25% infection rate for New York City which is suggested by antibody tests is actually the outer bound of how many infections a region could have before it peters out due to not having enough non-immune hosts left available. (For comparison, estimates are that it was about 25% of the US population that got Spanish Flu back in 1918 as well.) And say that the 0.5% infection fatality rate that suggests given New York City's death numbers is also correct. 330M times 25% times 0.5% is 412,000 deaths. Let's take that as our low number. For a mid number, let's assume that NYC is actually not at the maximum saturation point for infections. Maybe if we pretty much went about our normal lives about 40% of the population would get the virus. If we assume 40% infections and 0.5% mortality, we get 660,000 deaths. For our worst case scenario, let's imagine a 40% infection rate but also that the fatality rate that I'm estimating is a bit low. What if it's more like 1%, which I think is about the upper bound of the reasonable infection fatality rates that I've seen. Those assumptions get us to 1,320,000 deaths.
So if we hadn't done all this to try to stop the spread of the virus, there's a pretty decent possibility that we would be facing 400k to 1.3M deaths. I think we could all agree that's a really large number, and one it would be reasonable to take some pretty drastic actions to avoid. If the actions we're taking can reduce those down to something in the 100k to 200k range, it seems like that would be a potentially reasonable course of action. (I want to examine in depth the question of whether "lockdowns" actually save lives or just space them out over more time, but I think that needs its own post.)
However, a counter-argument that is often made is that while COVID-19 causes a lot of deaths, those are actually deaths that would have occurred soon anyway. According to this argument, the virus is mostly killing people who are very old and/or have existing conditions that put them in fragile health.
This is to some extent true. Here's a shot of the COVID-19 dashboard for my state of Ohio. I think it does a really good job of showing the dynamics of the virus:

So what does this mean in terms of the actual chance that people with COVID-19 will end up in the hospital or will end up dead? As we discussed earlier, lots of people who have the virus have not actually been tested, so the case numbers don't tell us everything. I also said that 0.5% overall fatality rate for all infections (not just identified cases) seems like a pretty plausible number based on the antibody studies from New York City. So here I've taken the Ohio population, assumed that actual infections are evenly distributed across the population even though the very mild nature of the disease in younger people means that fewer cases have been identified among the younger age groups, and projected an estimated total number of infections based on a total population IFR of 0.5%. (In other words, I first calculated that there were 367,200 infections by assuming that the 1,836 deaths represented a 0.5% IFR, and then spread those infections across the age groups based on the percent of Ohio residents in each age group.)
Well, for a lot of people the virus does give no symptoms at all or very mild symptoms. But keep in mind, we have a lot of people in our country. There are 12.5M people over 80 in the US. Apply these rates across the whole US population and you get to some large numbers. Let's go back to our minimum scenario where 25% of the US population got the virus. What would these hospitalization rates and fatality rates mean in terms of total deaths for different age groups? What I've done here is calculated 25% of the US population as the total number of infections and then distributed those infections evenly across the population according to how many people are in each age group. Obviously, there are a lot of assumptions being made here, but as a conservative scenario I don't think it's unreasonable.

But as we think about how much people would want to avoid getting this disease, how much they would stay away from restaurants and big gatherings in order to stay healthy even if not ordered to, and slow down the consumer economy as they did so, it's worth looking at the other set of estimates. Someone in his forties is almost a hundred times less likely to die if infected with the virus as someone who is 80+, but he's still a sixth as likely to end up in the hospital. While my estimate is that if 25% of Americans got the coronavirus, only 90,000 people under 70 would die of it, over 700,000 people under 70 would spend time in the hospital. Indeed, while 75% of the deaths would be people over 70, more than 60% the people hospitalized would be people under 70. 20% of the people hospitalized would be under fifty. 10% of people hospitalized would be under forty. I think we have to assume that there would be lots of other people who never ended up in hospitals but who felt really, really sick and scared for a couple weeks as they waited to see if they'd end up having to go to the hospital.
There are a lot of things that we don't know about this virus, and there are a lot of things we can reasonably argue about in how to respond to it. However, I think that this examination of the numbers underlines that while there have definitely been panicked numbers thrown around by people who didn't know what they were doing (I don't think that claims we'd see 5-10 million deaths ever fit well with what we knew, even back in February) this is a serious disease which, if left unchecked, could be responsible for a lot of deaths and a great deal of suffering. Hopefully this provides some insight into just what the dimensions of those possibilities are (and aren't.)
In my next post, I'll talk about the measures that have been taken to suppress the virus, including the "lockdowns" which are the subject of so much political dispute.
Saturday, May 16, 2020
Understanding the COVID-19 Outbreak: Part 3
This is the third part in a series. You can find the first part here and the second part here.
What Is A Pandemic Anyway?
My father-in-law tells a story about the day in high school that the football coach had to take over teaching Earth Science. He went up to the chalk board and began to write definitions. First up. "Lava flow" He considered a moment, then wrote the definition "Flow of lava".
I had a similarly recursive feeling when trying to look up definitions of "epidemic" and "pandemic" a while back in order to address the question of whether the coronavirus was really a pandemic. What is an epidemic? A disease that affects a large number of people in a region. What's a pandemic? An epidemic that spreads throughout the world. The CDC expresses it most succinctly of all: "A pandemic is a global outbreak of disease."
 And yet words like "pandemic" and "epidemic" and "plague" carry a set of implications that cause many people to engage their mental yardsticks. I've heard many people express sentiments to the effect of, "If this is a real pandemic, why aren't the bodies piling up like in the Black Death?" The Black Death is a sort of core myth of Western culture at this point for epidemic, complete with the Monty Python image of people trundling along with carts calling "Bring out your dead!" It's a terrible, terrible disease (which is still out there and occurs in about 5,000 people a year globally, though it can now be treated with anti-biotics) but it is only one of a huge number of infectious diseases which used to account for the majority of human deaths.
And yet words like "pandemic" and "epidemic" and "plague" carry a set of implications that cause many people to engage their mental yardsticks. I've heard many people express sentiments to the effect of, "If this is a real pandemic, why aren't the bodies piling up like in the Black Death?" The Black Death is a sort of core myth of Western culture at this point for epidemic, complete with the Monty Python image of people trundling along with carts calling "Bring out your dead!" It's a terrible, terrible disease (which is still out there and occurs in about 5,000 people a year globally, though it can now be treated with anti-biotics) but it is only one of a huge number of infectious diseases which used to account for the majority of human deaths.
If you look up the leading causes of death in the US at this time in history, you get the following list:
 Influenza and Pneumonia topped the list, followed by Tuberculosis. All infectious diseases of different sorts. Why is influenza less of a killer now? For the same reason that tuberculosis and pneumonia are, to an extent. The influenza virus is not always the primary killer. Often it weakens the body and immune system which allows bacterial pneumonia to take over and finish the patient off. With modern antibiotics we can treat those bacterial pneumonias thus lessening the death rate of influenza. Additionally, we have the influenza vaccines which build the body's resistance to the virus strains themselves and we have antiviral medications which can help to some extent.
Influenza and Pneumonia topped the list, followed by Tuberculosis. All infectious diseases of different sorts. Why is influenza less of a killer now? For the same reason that tuberculosis and pneumonia are, to an extent. The influenza virus is not always the primary killer. Often it weakens the body and immune system which allows bacterial pneumonia to take over and finish the patient off. With modern antibiotics we can treat those bacterial pneumonias thus lessening the death rate of influenza. Additionally, we have the influenza vaccines which build the body's resistance to the virus strains themselves and we have antiviral medications which can help to some extent.
But influenza and other infectious diseases were fully capable of killing lots of people, and that was just in a normal time when there wasn't an epidemic on the loose.
What makes an epidemic different from run of the mill "endemic" disease? It's not necessarily that that disease is spectacularly deadly. A disease is epidemic when it is spreading through the population rapidly and infecting a large number of them. In theory this could happen with some fairly minor disease, so long as it was quite contagious and not many people have antibodies that protected them from it. The difference is just that if a minor sniffle spread rapidly through the whole population, we wouldn't notice it a great deal.
The point about people not having antibodies that protect them from the disease is key. Diseases are, after all, essentially parasites. A virus can't reproduce all on its own. It needs to take over the cell of another creature and commandeer that cell to manufacture copies of itself. Once the body recognizes a virus for what it is, a hostile invader, the body develops antibodies that destroy the virus. So imagine that I have a virus that's colonized my body and is using my cells to crank out copies of itself. I'm coughing out micro-droplets of water vapor which contain those viruses. But all the people I come in contact with are people who have already come in contact with that type of virus, and as soon as one of the viruses comes into one of these bodies, the antibodies destroy it. So even though the viruses that have taken over my body are cranking out copies of themselves, they can't successfully colonize any other bodies. After a couple weeks, my body too develops good enough defenses to start attacking the virus, and so my body wipes out the infestation of viruses in my body and it's the end of the line for that strain of viruses because they weren't able to colonize the bodies of any other people I came into contact with.
With an endemic virus, a common virus that's been around for a while in the population, a lot of the people the virus comes in contact with are already able to fight the virus off, and so spread is slow. We can see how that is important when we look at times when endemic diseases became epidemic diseases because they came in contact with a new population. After Europeans reached the new world, diseases that were common in Europe (measles, smallpox, influenza, etc.) but which had not before been present in the Americas suddenly turned into epidemics. Measles was not an epidemic disease in Europe. It has highly contagious, but lots of people had had it before and were immune. Even children who hadn't had it before received some antibodies from their mothers during pregnancy and nursing, giving their bodies a head start when they encountered the virus for the first time. But in the Americas, measles was totally unknown. The result was that what in Europe was a bad but survivable childhood disease became in the Americas a population decimating epidemic. Much the same happened with other diseases that had been common in Europe but not in the Americas.
That there were so many diseases that were common in Europe but not in the Americas is believed to be due to the fact that Europeans had domesticated many more animals and lived in close contact with them. Many viruses first jump to the human population via a mutation of some animal virus. For instance, the flu virus which caused the deadly 1918 Spanish Flu pandemic is believed to have jumped from swine to humans in Kansas in the spring of 1918. If you want to read lots of interesting discussion about virus mutation, immunities, and pandemics, I'd recommend John Barry's The Great Influenza which I've been reading and finding fascinating.
When a new strain of an existing family of viruses (such as the 1918 Spanish Flu strain of the influenza virus) appears via mutation and/or jumping from some animal species to humans, if it is different enough from other strains that the immune system does not recognize it, the virus can spread rapidly in much the way that these new diseases did in the new world. But even the case of a "novel" virus (such as the novel coronavirus that we're dealing with now) there can still be degrees of susceptibility. The 1918 influenza pandemic was a novel strain which was significantly more deadly than normal seasonal flu. Seasonal flu kills around 0.1% of those who get it. In 1918, the fatality rate was more like 2.5%, twenty-five times higher than "normal" flu strains. Moreover, while seasonal influenza mostly kills those we'd think of as medically fragile (infants and old/infirm people) the 1918 flu hit people in their 20s and 30s particularly hard. And while all lives are of equal worth, it's not unreasonable that people would consider particularly tragic a disease which suddenly cuts down healthy young people who appeared to have their whole lives before them. But that 2.5% fatality rate was not consistent everywhere. The fatality rate was much higher among isolated populations that had seldom been exposed to other strains of flu. For instance, Inuit villages in Alaska and Canada in many cases experienced much higher death rates, sometimes near 100%. The same was the case for Pacific Islander populations, Australian Aborigines, etc. It's believed that the reason for this is that populations which had experienced fewer outbreaks of other flu stains were even more defenseless against the virus that populations where people's immune systems had at least identified and fought off other flu strains. Even though this particular stain was novel enough that everyone was susceptible to it, the familiarity with other flu strains somehow gave the immune system enough of an edge that it was able to build its defenses more quickly.
Although SARS-CoV-2 is a "novel virus", it may be that exposure to other types of corona viruses is one of the things which causes some people to suffer little or not sickness from the virus, developing antibodies that can fight off the virus without the body suffering much of any damage first, while other people experience a long, difficult, or even fatal respiratory disease.
So is COVID-19 a pandemic? Well, it is a rapid outbreak of a disease which has spread across the world. It first appeared in China and has now infected significant numbers of people in Iran, throughout Europe, the US, Canada, Mexico, Brazil, Ecuador, Turkey, Israel, India, the list goes on.
But as I said earlier, we could imagine a situation in which a disease was new enough that it swept across the world but in which the disease was not really that serious. What are we to say to the people who argue that COVID-19 isn't really killing many people, perhaps no more than an ordinary flu season?
I'd meant to get into the numbers question in this installment, but talking about the nature of pandemics took me longer than expected so I'll address numbers in the next installment, and at I'll also include a section of a the closely related topics: "lockdowns" and whether they have slowed the virus at all.
Click here for Part 4.
What Is A Pandemic Anyway?
My father-in-law tells a story about the day in high school that the football coach had to take over teaching Earth Science. He went up to the chalk board and began to write definitions. First up. "Lava flow" He considered a moment, then wrote the definition "Flow of lava".
I had a similarly recursive feeling when trying to look up definitions of "epidemic" and "pandemic" a while back in order to address the question of whether the coronavirus was really a pandemic. What is an epidemic? A disease that affects a large number of people in a region. What's a pandemic? An epidemic that spreads throughout the world. The CDC expresses it most succinctly of all: "A pandemic is a global outbreak of disease."

If you look up the leading causes of death in the US at this time in history, you get the following list:
Heart disease: 647,457Influenza and pneumonia are the only infectious diseases on the list, and they're ranked 8th out of 10. It didn't used to be this way. A New England Journal of Medicine Piece provides this comparison of what people died of in 1900 vs 2010.
Cancer: 599,108
Accidents (unintentional injuries): 169,936
Chronic lower respiratory diseases: 160,201
Stroke (cerebrovascular diseases): 146,383
Alzheimer’s disease: 121,404
Diabetes: 83,564
Influenza and pneumonia: 55,672
Nephritis, nephrotic syndrome, and nephrosis: 50,633
Intentional self-harm (suicide): 47,173

But influenza and other infectious diseases were fully capable of killing lots of people, and that was just in a normal time when there wasn't an epidemic on the loose.
What makes an epidemic different from run of the mill "endemic" disease? It's not necessarily that that disease is spectacularly deadly. A disease is epidemic when it is spreading through the population rapidly and infecting a large number of them. In theory this could happen with some fairly minor disease, so long as it was quite contagious and not many people have antibodies that protected them from it. The difference is just that if a minor sniffle spread rapidly through the whole population, we wouldn't notice it a great deal.
The point about people not having antibodies that protect them from the disease is key. Diseases are, after all, essentially parasites. A virus can't reproduce all on its own. It needs to take over the cell of another creature and commandeer that cell to manufacture copies of itself. Once the body recognizes a virus for what it is, a hostile invader, the body develops antibodies that destroy the virus. So imagine that I have a virus that's colonized my body and is using my cells to crank out copies of itself. I'm coughing out micro-droplets of water vapor which contain those viruses. But all the people I come in contact with are people who have already come in contact with that type of virus, and as soon as one of the viruses comes into one of these bodies, the antibodies destroy it. So even though the viruses that have taken over my body are cranking out copies of themselves, they can't successfully colonize any other bodies. After a couple weeks, my body too develops good enough defenses to start attacking the virus, and so my body wipes out the infestation of viruses in my body and it's the end of the line for that strain of viruses because they weren't able to colonize the bodies of any other people I came into contact with.
With an endemic virus, a common virus that's been around for a while in the population, a lot of the people the virus comes in contact with are already able to fight the virus off, and so spread is slow. We can see how that is important when we look at times when endemic diseases became epidemic diseases because they came in contact with a new population. After Europeans reached the new world, diseases that were common in Europe (measles, smallpox, influenza, etc.) but which had not before been present in the Americas suddenly turned into epidemics. Measles was not an epidemic disease in Europe. It has highly contagious, but lots of people had had it before and were immune. Even children who hadn't had it before received some antibodies from their mothers during pregnancy and nursing, giving their bodies a head start when they encountered the virus for the first time. But in the Americas, measles was totally unknown. The result was that what in Europe was a bad but survivable childhood disease became in the Americas a population decimating epidemic. Much the same happened with other diseases that had been common in Europe but not in the Americas.
That there were so many diseases that were common in Europe but not in the Americas is believed to be due to the fact that Europeans had domesticated many more animals and lived in close contact with them. Many viruses first jump to the human population via a mutation of some animal virus. For instance, the flu virus which caused the deadly 1918 Spanish Flu pandemic is believed to have jumped from swine to humans in Kansas in the spring of 1918. If you want to read lots of interesting discussion about virus mutation, immunities, and pandemics, I'd recommend John Barry's The Great Influenza which I've been reading and finding fascinating.
When a new strain of an existing family of viruses (such as the 1918 Spanish Flu strain of the influenza virus) appears via mutation and/or jumping from some animal species to humans, if it is different enough from other strains that the immune system does not recognize it, the virus can spread rapidly in much the way that these new diseases did in the new world. But even the case of a "novel" virus (such as the novel coronavirus that we're dealing with now) there can still be degrees of susceptibility. The 1918 influenza pandemic was a novel strain which was significantly more deadly than normal seasonal flu. Seasonal flu kills around 0.1% of those who get it. In 1918, the fatality rate was more like 2.5%, twenty-five times higher than "normal" flu strains. Moreover, while seasonal influenza mostly kills those we'd think of as medically fragile (infants and old/infirm people) the 1918 flu hit people in their 20s and 30s particularly hard. And while all lives are of equal worth, it's not unreasonable that people would consider particularly tragic a disease which suddenly cuts down healthy young people who appeared to have their whole lives before them. But that 2.5% fatality rate was not consistent everywhere. The fatality rate was much higher among isolated populations that had seldom been exposed to other strains of flu. For instance, Inuit villages in Alaska and Canada in many cases experienced much higher death rates, sometimes near 100%. The same was the case for Pacific Islander populations, Australian Aborigines, etc. It's believed that the reason for this is that populations which had experienced fewer outbreaks of other flu stains were even more defenseless against the virus that populations where people's immune systems had at least identified and fought off other flu strains. Even though this particular stain was novel enough that everyone was susceptible to it, the familiarity with other flu strains somehow gave the immune system enough of an edge that it was able to build its defenses more quickly.
Although SARS-CoV-2 is a "novel virus", it may be that exposure to other types of corona viruses is one of the things which causes some people to suffer little or not sickness from the virus, developing antibodies that can fight off the virus without the body suffering much of any damage first, while other people experience a long, difficult, or even fatal respiratory disease.
So is COVID-19 a pandemic? Well, it is a rapid outbreak of a disease which has spread across the world. It first appeared in China and has now infected significant numbers of people in Iran, throughout Europe, the US, Canada, Mexico, Brazil, Ecuador, Turkey, Israel, India, the list goes on.
But as I said earlier, we could imagine a situation in which a disease was new enough that it swept across the world but in which the disease was not really that serious. What are we to say to the people who argue that COVID-19 isn't really killing many people, perhaps no more than an ordinary flu season?
I'd meant to get into the numbers question in this installment, but talking about the nature of pandemics took me longer than expected so I'll address numbers in the next installment, and at I'll also include a section of a the closely related topics: "lockdowns" and whether they have slowed the virus at all.
Click here for Part 4.
Friday, May 15, 2020
Charis in the World of Wonders, by Marly Youmans: A Review
I received a review copy of Charis in the World of Wonders, but my thoughts are all my own.
My Amazon review:
Gentle Charis, educated, red-haired, and the sole survivor of the massacre of her settlement, flees through the forests of the Massachusetts Bay Colony to rebuild her life in the more established towns near Boston. There she finds that the world holds other, subtler dangers than just the Mi'kmaq tribe and the French. Some Puritans are eager to see the judgment of God in the sufferings of others; some friendships end in grief. Sullen suspicions of witchcraft simmer around a girl who has escaped the dangers of the wild and who trusts that God seasons judgment with mercy.
Charis has heard old German fairytales, and echoes of those stories resonate in her own as she takes a position sewing for a dour widow with two headstrong daughters, who suspect the few precious possessions that remind her of her mother's care. But she also finds that the death of her family cannot kill love, and that grace and beauty are constantly breaking through the dull surface of the world, not least through a silversmith with silver eyes and golden hair.
Marly Youmans is a poet as well as a novelist, and her graceful prose sets Charis's terrors and joys in an authentic and sensitive historical voice. She weaves the strangely colorful language of the New England colonies into the story with a sure hand, and realizes the Puritans as a people of ecstatic vision of heaven as well as hell. (A glossary in the back of the book helps the reader over more obscure terms, though the reader may wish more for a map to trace Charis's wanderings.) The quiet lyricism and episodic pacing of the novel provides just enough distance from the sorrows of the story, as Charis wrestles with guilt and the trauma of her family's death, comforts an agonized new mother with no will to live, bears slander, and fears that once again she will have to flee from the world she knows into a wider world of wonders.
***
When I was asked if I would like a review copy of this novel, I was wary at first, because the promotional material I'd read was very vague and focused mostly on the poeticism (and other discerning readers have told me that they'd had the same hesitation). The novelist du jour of wonder is Marilynne Robinson, and terms of you can draw parallels between this novel and Robinson's Gilead in terms of realizing the wonder of the everyday world. However, I think I'd prefer a comparison with the novels of Ron Hansen, specifically Mariette in Ecstasy or Exiles. Ms. Youmans and Mr. Hansen share a deep commitment to moral questions not just pondered and wondered, but acted on even at the moment of mortal peril. Charis in the World of Wonders is a novel which demands real choices of the characters, in which wonder is not just a glistening opiate, but a sublime, dangerous glimpse of reality that demands a moral response.
Response, moral choice: these are key elements. I recently read The Diary of a Country Priest, by Georges Bernanos. This novel is classic Catholic literature, and it is very good, but large parts of it are characters laying out to one another their religious and political philosophies. There's nothing wrong with that, necessarily, but the language of the pressing discourse and class concerns of 1936 France can seem quaintly distant to readers of 2020. Bernanos was, of course, writing a contemporary novel, not trying to make historical debates relevant to a future audience. (The spiritual grapplings of the main character could also grow a bit wearing for the reader, who realizes that the priest's spiritual agonies are more than a little influenced by his deteriorating health, and that a good rest in a sanatorium might be more spiritually beneficial to a clearly dying man than one more disquisition about the state of the French worker.)
But as I skimmed one multi-page monologue after another, I found myself yearning for the moments of choice -- the moments when the grand philosophies and the agonized doubts played out, and people had to act on their convictions. And those moments were gripping. Indeed, the last page of the novel, describing how the priest faced a painful lonely death, is worth the whole rest of the book. It is what he truly believes, lived.
And so with Charis. There are necessary interludes where characters must grapple with pressing questions: did God ordain the deaths of my family? Are my sufferings a judgment on me? Is survival a mark of grace or a sign of diabolical alliance? And then Charis must accept grace and extend it to others, the small internal struggles no less dramatically significant than the external adventures. The comparison to Cinderella is apt, I think: grace is not less costly for being quiet and outwardly insignificant.
But when we speak of novels, we are also speaking of literary merits, and it is often the downfall of religious novels that the best of moral intentions become heavy-handed and didactic without literary ability. (And ability is often underserved without the attentions of an editor attuned as much to style as consistency and editorial guidelines.) So I am very pleased to see any Catholic publisher bringing out a novel by an established author with a sure literary style, and who sticks the ending. As anyone who has read any quantity of religion-adjacent fiction can testify, these qualities are by no means assured, and the difficulty of finding excellent new fiction is compounded by the tendency of reviewers to give a pass to literary merits to members of the tribe.
Ms. Youmans, as mentioned above, is a poet, and I'm aware that I myself am inclined to a plainer style. There were, to me, moments when poeticism threatened to undermine the narration. A small example: a pregnant character says of her child that "He clenches together and opens up like a thread of metal coiled up and pressed and released." That is a lot of words to describe a spring. If such a concept did not exist in the late 17th century, it would be exceedingly odd to invent it in this way. (Wikipedia informs me that coiled springs do indeed date back to the 15th century.) But more to the point, it was an overly complex image that drew too much attention to itself.
Why nitpick in this way? Because I think this is an excellent novel with few flaws, and I want to you trust that I read it and am giving you an honest review. I'd like to commend Ignatius Press for bringing out an important novel that deserves a place with any of the literary fiction coming from the major publisher, in a handsome edition with original artistic motifs at the head of each chapter. If anything is going to rebuild readers' trust in the inbred Catholic fiction industry, it will be a fierce attention to literary as well as moral integrity.
When I was asked if I would like a review copy of this novel, I was wary at first, because the promotional material I'd read was very vague and focused mostly on the poeticism (and other discerning readers have told me that they'd had the same hesitation). The novelist du jour of wonder is Marilynne Robinson, and terms of you can draw parallels between this novel and Robinson's Gilead in terms of realizing the wonder of the everyday world. However, I think I'd prefer a comparison with the novels of Ron Hansen, specifically Mariette in Ecstasy or Exiles. Ms. Youmans and Mr. Hansen share a deep commitment to moral questions not just pondered and wondered, but acted on even at the moment of mortal peril. Charis in the World of Wonders is a novel which demands real choices of the characters, in which wonder is not just a glistening opiate, but a sublime, dangerous glimpse of reality that demands a moral response.
Response, moral choice: these are key elements. I recently read The Diary of a Country Priest, by Georges Bernanos. This novel is classic Catholic literature, and it is very good, but large parts of it are characters laying out to one another their religious and political philosophies. There's nothing wrong with that, necessarily, but the language of the pressing discourse and class concerns of 1936 France can seem quaintly distant to readers of 2020. Bernanos was, of course, writing a contemporary novel, not trying to make historical debates relevant to a future audience. (The spiritual grapplings of the main character could also grow a bit wearing for the reader, who realizes that the priest's spiritual agonies are more than a little influenced by his deteriorating health, and that a good rest in a sanatorium might be more spiritually beneficial to a clearly dying man than one more disquisition about the state of the French worker.)
But as I skimmed one multi-page monologue after another, I found myself yearning for the moments of choice -- the moments when the grand philosophies and the agonized doubts played out, and people had to act on their convictions. And those moments were gripping. Indeed, the last page of the novel, describing how the priest faced a painful lonely death, is worth the whole rest of the book. It is what he truly believes, lived.
And so with Charis. There are necessary interludes where characters must grapple with pressing questions: did God ordain the deaths of my family? Are my sufferings a judgment on me? Is survival a mark of grace or a sign of diabolical alliance? And then Charis must accept grace and extend it to others, the small internal struggles no less dramatically significant than the external adventures. The comparison to Cinderella is apt, I think: grace is not less costly for being quiet and outwardly insignificant.
But when we speak of novels, we are also speaking of literary merits, and it is often the downfall of religious novels that the best of moral intentions become heavy-handed and didactic without literary ability. (And ability is often underserved without the attentions of an editor attuned as much to style as consistency and editorial guidelines.) So I am very pleased to see any Catholic publisher bringing out a novel by an established author with a sure literary style, and who sticks the ending. As anyone who has read any quantity of religion-adjacent fiction can testify, these qualities are by no means assured, and the difficulty of finding excellent new fiction is compounded by the tendency of reviewers to give a pass to literary merits to members of the tribe.
Ms. Youmans, as mentioned above, is a poet, and I'm aware that I myself am inclined to a plainer style. There were, to me, moments when poeticism threatened to undermine the narration. A small example: a pregnant character says of her child that "He clenches together and opens up like a thread of metal coiled up and pressed and released." That is a lot of words to describe a spring. If such a concept did not exist in the late 17th century, it would be exceedingly odd to invent it in this way. (Wikipedia informs me that coiled springs do indeed date back to the 15th century.) But more to the point, it was an overly complex image that drew too much attention to itself.
Why nitpick in this way? Because I think this is an excellent novel with few flaws, and I want to you trust that I read it and am giving you an honest review. I'd like to commend Ignatius Press for bringing out an important novel that deserves a place with any of the literary fiction coming from the major publisher, in a handsome edition with original artistic motifs at the head of each chapter. If anything is going to rebuild readers' trust in the inbred Catholic fiction industry, it will be a fierce attention to literary as well as moral integrity.
Wednesday, May 13, 2020
Understanding the COVID-19 Outbreak: Part 2
This is Part 2 of my big coronavirus analysis post. You can read Part 1 here.
What Is It About Coronavirus?
Let's pause for a moment at this point to talk about why this particular virus caused countries to do such destructive things to stop its spread. Why did China carry out a shutdown which is causing it to log negative GDP growth in its official numbers for the first time since it abandoned Maoist fantasy and joined the modern world? Some people have put forward theories that this is a Chinese conspiracy to cripple the West, or a liberal conspiracy to hurt Trump or an "elite" conspiracy to exert more control over the lives of the ordinary people. Within each country and culture there are various groups reacting to this situation for various reasons of their own, but I think it's hard to see the broad reaction throughout the world as being caused by something other than the virus itself. And why this virus?
There are scarier diseases in terms of symptoms. Ebola seems like classic horror movie material in what it does to the body. And of course, there's always good old fashioned bubonic plague to fill your nightmares. However, this particular coronavirus has a set of characteristics which fit a profile sufficient to make epidemiologists and those who listen to them fairly worried.
It's fairly contagious, with the ability to pass from person to person via tiny airborne droplets of water vapor expelled from the nose and mouth when coughing, speaking, breathing, etc. It has a one to two week incubation period during which the newly infected person is contagious and thus at risk of spreading the virus without even knowing yet that he is sick. It's not so deadly as to wipe out its host population before they can pass it on to others, but it is more deadly than widespread diseases such as seasonal flu.
 The SARS-CoV-2 virus which causes the disease known as COVID-19 (I must say, we are not very poetic givers of names these days) is not a malevolent force out to get us. It is a not-quite-living thing with a set of RNA code which can bond with a cell, take it over, and use the cell to manufacture duplicates of itself. In the process of thus hijacking cells, the virus often causes a good deal of damage to the body. This particular virus is particularly troublesome to us because it is different enough from other related viruses (called coronaviruses because of the "crown" of spiky proteins sticking out from the virus) that our bodies don't have ready-formed antibodies waiting to attack the invaders. This doesn't mean that it's impossible for our bodies to fight it off. Our bodies are constantly learning to identify new bacterial and viral invaders and producing new antibodies to fight them off. However, this process of getting a large enough infestation of some new disease for our bodies to successfully learn from the attack, build antibodies, and be ready to deal with any similar invaders who show up in the future is a process that we as whole humans often identify as "getting sick."
The SARS-CoV-2 virus which causes the disease known as COVID-19 (I must say, we are not very poetic givers of names these days) is not a malevolent force out to get us. It is a not-quite-living thing with a set of RNA code which can bond with a cell, take it over, and use the cell to manufacture duplicates of itself. In the process of thus hijacking cells, the virus often causes a good deal of damage to the body. This particular virus is particularly troublesome to us because it is different enough from other related viruses (called coronaviruses because of the "crown" of spiky proteins sticking out from the virus) that our bodies don't have ready-formed antibodies waiting to attack the invaders. This doesn't mean that it's impossible for our bodies to fight it off. Our bodies are constantly learning to identify new bacterial and viral invaders and producing new antibodies to fight them off. However, this process of getting a large enough infestation of some new disease for our bodies to successfully learn from the attack, build antibodies, and be ready to deal with any similar invaders who show up in the future is a process that we as whole humans often identify as "getting sick."
In the case of this new coronavirus, the getting sick part can involve no symptoms at all, or a set of symptoms like a bad flu, or a set of symptoms that land you in the hospital with low oxygen levels and trouble breathing, or in perhaps 1% to 0.5% of infections: symptoms that end up killing you. Which of these outcomes you get will depend a great deal on your age, your health, and any number of other circumstances that we don't yet fully understand.
And throughout the period during which coronaviruses are running around inside your body, hijacking cells and turning them into virus factories (while your body tools up to produce enough antibodies to wipe out the virus infestation) the newly produced viruses are finding their way into secretions in the lungs, throat, nose, and mouth which then float off through the air as little globules of moisture, which can in turn be breathed in by other people and allow the viruses that are along for the ride to colonize new cells in a new host body which doesn't yet have suitable antibodies. (If these semi-dramatized descriptions of battles going on within the body sound entertaining, your kids like ours may enjoy the Japanese animated series Cells At Work which can be found on Netflix, in which these sort of things are dramatized to the hilt.)
An important implication of all this description, which I'll get back to shortly when discussing "lockdowns" is that when we talk about how contagious a disease is, we're not talking about something which is a simple characteristic of the disease itself, but rather a result of a number of factors:
- how long the infected body is putting out viruses
- how many viruses the infected body is putting out and by what means those viruses might reach a new host
- how easily stray viruses can get into a new host body and form a viable infestation
- how often infected people are coming into contact with other people
- what percentage of people the infected host comes into contact with are themselves susceptible to infestation
If, on average, given the ability of an infected person to give off viruses and the ease with which those viruses can infect other people and how frequently people meet and how many of the people met are susceptible to infection, one infected person manages to pass the infection on to more than one other person before the infected person's body adapts and successfully wipes out the infection, the disease will continue to spread to a larger number of people and the outbreak will grow. If, on the other hand, the average infected person hands the disease on to less than one new host for the disease, the size of the outbreak will shrink. This measure of how many people the average infected person passes the infection on to is called the R(n) or R0 by epidemiologists. An R(n) which is above 1.0 means that the outbreak is spreading. One below 1.0 means it is shrinking.
COVID-19 Goes Global
The world these days is a pretty connected place, and the threads of those connections are many and tangled. If you had asked me last year where an infectious disease originating in China would spread next outside of Asia, my guess would not have been "Iran and then Italy" but that is the order of march which COVID-19 followed during January and February this year. The fact that the virus hopped from China to Iran and India reminds us that China does not just sell us cheap manufactured goods. China is working to make itself a power for development around the world, and as such they're busy acquiring companies and spreading consultants and business contacts through countries that might like an alternative to working with US companies.
It's been observed, and there's probably a fair amount of justice to this, that it was when the coronavirus outbreak in Italy got really bad that people in the US started to wake up and take notice. Yes, there are those who try to shrug off Italy as if it's a borderline third world country with a fragile health care system, but whatever stones one might choose to throw at Italy's political and medical establishments, we're talking about a modern, Western, affluent country. The hardest hit part of Italy (so far) is Lombardy, the northern province that includes the industrial powerhouse city of Milan. Logically, we should have taken it seriously back when it was hitting China, but there was still some sense in which people could imagine it was only "over there". Now the virus was decimating a European country.
There can be a lot of random chance in the early stages of a pandemic. One sick person goes from one city to another. Does he spend lots of time with many different people, or does he keep to himself? Does he ride the metro or take a taxi? Later on in the process it's a numbers game, but in the early stages spread can be very individual. Through whatever series of chances, Italy became central to the Western outbreak of COVID-19. On February 23rd, the Italian government shut down the Venetian Carnivale two days early, ending a major tourist event out of fears that continued gatherings would serve to spread the virus more. Looking back, having the scale of how big the outbreak would become for reference, it's perhaps impressive that they moved so fast. On Feb 23rd (according to the John Hopkins global dataset) Italy had 155 confirmed cases and 3 deaths. It wasn't until a couple weeks later on March 9th that Italy imposed a national "lockdown", asking people to stay in their homes except for essential work and errands. In those couple weeks, the counts had increased to just over 9,000 confirmed cases and nearly 500 dead. Italians took the lockdown order seriously, and indeed had been increasingly practicing "social distancing" (the phrase we now all know so well) in the period leading up to the order. However, because it takes around three weeks for someone who will eventually die of the virus to go from exposure to symptoms to death, it wasn't for another three weeks that the effects of that social distancing began to appear in the number of daily deaths leveling off and beginning to decrease.

However, although Italy copied the "lockdown" approach from China, it did not engage in the kind of aggressive tracing and quarantining of sick or exposed people that had been used by Asian nations in successfully crushing their outbreaks. The result is the lopsided curve that is seen above. What this shows is that Italy (in a pattern we've since seen in many other Western countries with major outbreaks) imposed restrictions severe enough to drastically slow the transmission of the virus, but not enough to actually wipe it out. (I performed some rudimentary modeling to demonstrate this dynamic a little while back.) Italy saw their peak daily deaths of just over 900 back on March 27th. As of that day, Italy had a cumulative 9,134 officially recorded COVID-19 deaths. (Actual death totals appear to be above the official numbers.) As of May 13th, the total officially recorded deaths are over 30,000 and still increasing by over 150 a day. With the shape of the outbreak curve, passing the peak doesn't yet mean that you're halfway through.
There were already individual cases of COVID-19 in the US and in other Western countries as the Italian outbreak got going. We now believe the first US death due to COVID-19 was back on February 6th the result of a West Cost strain of the virus which came directly from China. But it was from Italy that the virus spread out across Europe and to New York City. And although the US had already been seeded with strains of the virus which had come with travelers directly from China, it is the New York outbreak (based on the strains which circulated in Europe) which has spread throughout the US and is the predominant source the other regional outbreaks in the US.
The US outbreak gets the lion's share of attention in our US media, partly because it's the local story, and partly because it's the "biggest". However, it's worth noting that one reason the US outbreak is the biggest is simply that the US is very big. If you look at the number of COVID-19 deaths per 1M of population, the US is high but definitely not the highest. That sad honor currently goes to Belgium, whose outbreak (due to peaking later than Italy and Spain, and not having the political implications of the outbreaks in the US and UK) doesn't get as much press.
 But of course, even this is a bit of a simplistic view, because the US outbreak is really a number of highly regional outbreaks. The biggest by far is in the New York area, and if you look at New York State as if it were its own country, it would have the deadliest outbreak of any in the world. If we take some US states and mix them in with countries, all sorts of interesting comparisons arise.
But of course, even this is a bit of a simplistic view, because the US outbreak is really a number of highly regional outbreaks. The biggest by far is in the New York area, and if you look at New York State as if it were its own country, it would have the deadliest outbreak of any in the world. If we take some US states and mix them in with countries, all sorts of interesting comparisons arise.
 New York is almost twice as bad as Belgium, with New Jersey and Connecticut also having worse outbreaks than any European country. Louisiana is neck and neck with Italy. Ohio is better than Canada and Ecuador but worse than Germany. Florida is better than Denmark but worse than Iran. Texas has had a slightly less deadly outbreak so far than Norway.
New York is almost twice as bad as Belgium, with New Jersey and Connecticut also having worse outbreaks than any European country. Louisiana is neck and neck with Italy. Ohio is better than Canada and Ecuador but worse than Germany. Florida is better than Denmark but worse than Iran. Texas has had a slightly less deadly outbreak so far than Norway.
As all these countries have dealt with their outbreaks, they've mostly pursued the same "lockdown" policies, and they've all seen the same sorts of lopsided curves with a sharp increase at the beginning and a long slow decline at after the peak. The big exception is Sweden, which has asked its citizens to voluntarily pursue social distancing but has not imposed government lockdowns. These lockdowns have become a key area of controversy which I'll address in a later section. In the next section, however, I'd like to address the question of how we measure the coronavirus outbreak and get some sense of how serious it is.
Continued: Read Part 3
What Is It About Coronavirus?
Let's pause for a moment at this point to talk about why this particular virus caused countries to do such destructive things to stop its spread. Why did China carry out a shutdown which is causing it to log negative GDP growth in its official numbers for the first time since it abandoned Maoist fantasy and joined the modern world? Some people have put forward theories that this is a Chinese conspiracy to cripple the West, or a liberal conspiracy to hurt Trump or an "elite" conspiracy to exert more control over the lives of the ordinary people. Within each country and culture there are various groups reacting to this situation for various reasons of their own, but I think it's hard to see the broad reaction throughout the world as being caused by something other than the virus itself. And why this virus?
There are scarier diseases in terms of symptoms. Ebola seems like classic horror movie material in what it does to the body. And of course, there's always good old fashioned bubonic plague to fill your nightmares. However, this particular coronavirus has a set of characteristics which fit a profile sufficient to make epidemiologists and those who listen to them fairly worried.
It's fairly contagious, with the ability to pass from person to person via tiny airborne droplets of water vapor expelled from the nose and mouth when coughing, speaking, breathing, etc. It has a one to two week incubation period during which the newly infected person is contagious and thus at risk of spreading the virus without even knowing yet that he is sick. It's not so deadly as to wipe out its host population before they can pass it on to others, but it is more deadly than widespread diseases such as seasonal flu.

In the case of this new coronavirus, the getting sick part can involve no symptoms at all, or a set of symptoms like a bad flu, or a set of symptoms that land you in the hospital with low oxygen levels and trouble breathing, or in perhaps 1% to 0.5% of infections: symptoms that end up killing you. Which of these outcomes you get will depend a great deal on your age, your health, and any number of other circumstances that we don't yet fully understand.
And throughout the period during which coronaviruses are running around inside your body, hijacking cells and turning them into virus factories (while your body tools up to produce enough antibodies to wipe out the virus infestation) the newly produced viruses are finding their way into secretions in the lungs, throat, nose, and mouth which then float off through the air as little globules of moisture, which can in turn be breathed in by other people and allow the viruses that are along for the ride to colonize new cells in a new host body which doesn't yet have suitable antibodies. (If these semi-dramatized descriptions of battles going on within the body sound entertaining, your kids like ours may enjoy the Japanese animated series Cells At Work which can be found on Netflix, in which these sort of things are dramatized to the hilt.)
An important implication of all this description, which I'll get back to shortly when discussing "lockdowns" is that when we talk about how contagious a disease is, we're not talking about something which is a simple characteristic of the disease itself, but rather a result of a number of factors:
- how long the infected body is putting out viruses
- how many viruses the infected body is putting out and by what means those viruses might reach a new host
- how easily stray viruses can get into a new host body and form a viable infestation
- how often infected people are coming into contact with other people
- what percentage of people the infected host comes into contact with are themselves susceptible to infestation
If, on average, given the ability of an infected person to give off viruses and the ease with which those viruses can infect other people and how frequently people meet and how many of the people met are susceptible to infection, one infected person manages to pass the infection on to more than one other person before the infected person's body adapts and successfully wipes out the infection, the disease will continue to spread to a larger number of people and the outbreak will grow. If, on the other hand, the average infected person hands the disease on to less than one new host for the disease, the size of the outbreak will shrink. This measure of how many people the average infected person passes the infection on to is called the R(n) or R0 by epidemiologists. An R(n) which is above 1.0 means that the outbreak is spreading. One below 1.0 means it is shrinking.
COVID-19 Goes Global
The world these days is a pretty connected place, and the threads of those connections are many and tangled. If you had asked me last year where an infectious disease originating in China would spread next outside of Asia, my guess would not have been "Iran and then Italy" but that is the order of march which COVID-19 followed during January and February this year. The fact that the virus hopped from China to Iran and India reminds us that China does not just sell us cheap manufactured goods. China is working to make itself a power for development around the world, and as such they're busy acquiring companies and spreading consultants and business contacts through countries that might like an alternative to working with US companies.
It's been observed, and there's probably a fair amount of justice to this, that it was when the coronavirus outbreak in Italy got really bad that people in the US started to wake up and take notice. Yes, there are those who try to shrug off Italy as if it's a borderline third world country with a fragile health care system, but whatever stones one might choose to throw at Italy's political and medical establishments, we're talking about a modern, Western, affluent country. The hardest hit part of Italy (so far) is Lombardy, the northern province that includes the industrial powerhouse city of Milan. Logically, we should have taken it seriously back when it was hitting China, but there was still some sense in which people could imagine it was only "over there". Now the virus was decimating a European country.
There can be a lot of random chance in the early stages of a pandemic. One sick person goes from one city to another. Does he spend lots of time with many different people, or does he keep to himself? Does he ride the metro or take a taxi? Later on in the process it's a numbers game, but in the early stages spread can be very individual. Through whatever series of chances, Italy became central to the Western outbreak of COVID-19. On February 23rd, the Italian government shut down the Venetian Carnivale two days early, ending a major tourist event out of fears that continued gatherings would serve to spread the virus more. Looking back, having the scale of how big the outbreak would become for reference, it's perhaps impressive that they moved so fast. On Feb 23rd (according to the John Hopkins global dataset) Italy had 155 confirmed cases and 3 deaths. It wasn't until a couple weeks later on March 9th that Italy imposed a national "lockdown", asking people to stay in their homes except for essential work and errands. In those couple weeks, the counts had increased to just over 9,000 confirmed cases and nearly 500 dead. Italians took the lockdown order seriously, and indeed had been increasingly practicing "social distancing" (the phrase we now all know so well) in the period leading up to the order. However, because it takes around three weeks for someone who will eventually die of the virus to go from exposure to symptoms to death, it wasn't for another three weeks that the effects of that social distancing began to appear in the number of daily deaths leveling off and beginning to decrease.

However, although Italy copied the "lockdown" approach from China, it did not engage in the kind of aggressive tracing and quarantining of sick or exposed people that had been used by Asian nations in successfully crushing their outbreaks. The result is the lopsided curve that is seen above. What this shows is that Italy (in a pattern we've since seen in many other Western countries with major outbreaks) imposed restrictions severe enough to drastically slow the transmission of the virus, but not enough to actually wipe it out. (I performed some rudimentary modeling to demonstrate this dynamic a little while back.) Italy saw their peak daily deaths of just over 900 back on March 27th. As of that day, Italy had a cumulative 9,134 officially recorded COVID-19 deaths. (Actual death totals appear to be above the official numbers.) As of May 13th, the total officially recorded deaths are over 30,000 and still increasing by over 150 a day. With the shape of the outbreak curve, passing the peak doesn't yet mean that you're halfway through.
There were already individual cases of COVID-19 in the US and in other Western countries as the Italian outbreak got going. We now believe the first US death due to COVID-19 was back on February 6th the result of a West Cost strain of the virus which came directly from China. But it was from Italy that the virus spread out across Europe and to New York City. And although the US had already been seeded with strains of the virus which had come with travelers directly from China, it is the New York outbreak (based on the strains which circulated in Europe) which has spread throughout the US and is the predominant source the other regional outbreaks in the US.
The US outbreak gets the lion's share of attention in our US media, partly because it's the local story, and partly because it's the "biggest". However, it's worth noting that one reason the US outbreak is the biggest is simply that the US is very big. If you look at the number of COVID-19 deaths per 1M of population, the US is high but definitely not the highest. That sad honor currently goes to Belgium, whose outbreak (due to peaking later than Italy and Spain, and not having the political implications of the outbreaks in the US and UK) doesn't get as much press.

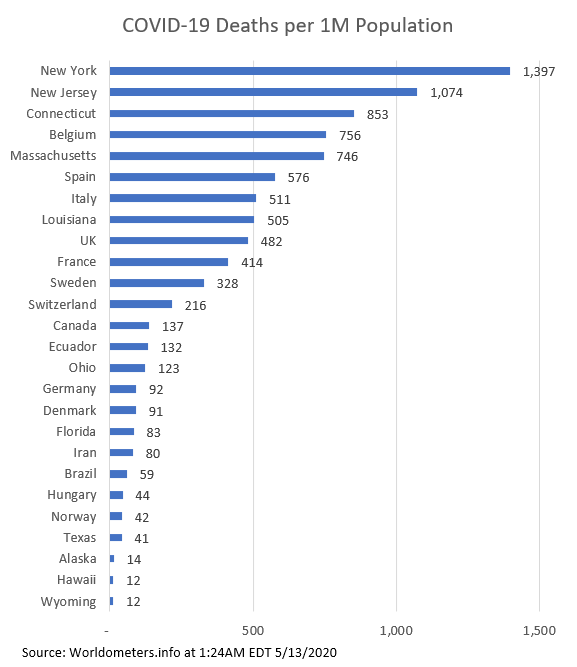
As all these countries have dealt with their outbreaks, they've mostly pursued the same "lockdown" policies, and they've all seen the same sorts of lopsided curves with a sharp increase at the beginning and a long slow decline at after the peak. The big exception is Sweden, which has asked its citizens to voluntarily pursue social distancing but has not imposed government lockdowns. These lockdowns have become a key area of controversy which I'll address in a later section. In the next section, however, I'd like to address the question of how we measure the coronavirus outbreak and get some sense of how serious it is.
Continued: Read Part 3
Understanding the COVID-19 Outbreak: Part 1
For reasons of length, this post has had to be broken into multiple parts.
The coronavirus outbreak and the way that it's been dealt with by our country is such a big topic that even though I've been following the story a great deal and trying to understand it, writing comprehensively on the topic seems daunting. And yet, it's trying to fit the entire topic together in some sort of context that seems most needed. Thus, this post will attempt to tackle first how I came to think about the topic the way I do, and then my understanding where we are, how we got here, and where we may be going.
How I Got This Way
I heard about the coronavirus fairly early (mid-January) because the company I work for has offices in China and in Taiwan, and so we had colleagues who were affected by the Chinese lockdown and travel restrictions back in January. I also knew from seeing the dramatic slowdown in sales to our Chinese customers (and from my Chinese colleagues who were working from home despite being over five hundred miles from Wuhan) that China was making a massive effort to contain the virus and that that was likely to have significant economic effects.
And yet, I was blind to the possibility that we would actually end up with a significant outbreak in the US. Looking back, there wasn't any rational basis for this blindness. Rather, there was a sort of habitual interpretive filter that we often apply instead of reason because it's quicker and easier. Various other outbreaks had occurred without becoming widespread in the US (SARS, MERS, Zika, Ebola, etc.) and so I made the assumption that somehow or other -- through luck or the efforts of epidemiologists or travel screening or the blessings of first world life we take for granted -- we wouldn't get more than a smattering of cases in the US.
It was in early March, as it began to become clear this was not the case, that I started to play catch up on reading about the virus. In my reading I was fortunate, in that the first people I looked to were people I knew to be scientifically and statistically literate. I quickly realized that Razib Kahn of the Gene Expression blog was taking the virus very seriously. Razib is someone I've been reading off and on for nearly fifteen years, almost since this blog began. His scientific work is in genetics, he's got a strong understanding of data analysis, and he's also very historically literate. Nor is he easily led by convention. (The NY Times at one point invited him to be a recurring contributor and then pulled the invitation because they decided he was too un-PC.) Another person whose thinking about the virus guided my early impressions was Josiah Neeley who ages ago was the libertarian voice on Vox Nova and wrote the Blackadder blog. Now you can hear him under his own name at the Urbane Cowboys podcast (which is one I try to listen to every week even though I don't like podcasts as a format.) If you want to hear my two main influences come together, Razib was a guest on the Urban Cowboys podcast in this episode back in March focusing on the coronavirus. Through them I found a number of people on twitter who seemed to be addressing the topic realistically and linking to good scientific content.
This was my background when I wrote my first post touching on an aspect of the coronavirus outbreak and the measures proposed to slow it's spread back on March 14th, which not-coincidentally was the day after my last day in the office at my employer, as those of us not working the manufacturing plant had all been told to work from home until further notice. (That I have a job I'm able to do from home and remain gainfully employed is a good fortune for which I am duly grateful, though the economic effects of the pandemic will still be hitting the company hard and thus we're dealing with pay cuts, etc. in order to keep the company solvent.)
But as I was learning about the situation, the situation and the response to it by various countries was changing rapidly. What are we to make of these developments?
Coronavirus: Origin Story
I have no intention of trying to dig into the question of how the virus got loose in the first place, as this is one of the things it will probably take us longest to have clear information about. What does seem pretty clear, however, is that China first went through a phase of trying to pretend the outbreak did not exist. While they're an oppressive autocracy, their instincts here were probably not that different from the instincts that have made more democratic governments deny the seriousness of the situation at first. They didn't want to scare people, admit possible incompetence, and suffer the economic disruption of a major disease outbreak, and so at first they hoped it would go away. It didn't. So China then went into a second phase of trying to actively suppress the disease. To that end, they shut down travel between the city of Wuhan (where the outbreak had originated) and other parts of China. They put people both inside and outside Hubei province under lockdown. And then within Wuhan itself (which is by population about the size of New York City, but is only the 9th most populous city in China) they began to enforce strict quarantines of all sick people and even of people who had been exposed to sick people. China being a repressive and secretive society, it's hard to know for sure what did and didn't happen, but there are rhumors that spread from China at the time about sick people being welded into their apartments and left to die.

Whether these darker stories are true or the CCP was merely pursuing a conventional but strict set of isolation rules, the result was that although by the end of January there had been cases identified in many parts of China as well as in nearby countries and even in the US, the virus never spread widely in Chinese provinces other than Hubei. Pulling down data from the John Hopkins data portal, and charting the number of reported new cases each day, Hubei frequently reported over a thousand new cases a day in late January and early February, while the other provinces with the largest outbreaks were reporting just over a hundred.
 Of course, that phrase "reported cases" is key. China is not a free society, and throughout the crisis the regime has acted to preserve its prestige. It may well be that China is lying to some extent about the number of cases and number of deaths. Even if they aren't intentionally lying, local officials may be hiding the truth from higher officials in order to make themselves look better. And of course, all countries' counts are suspect at this point because information is difficult to come by. There's no way to know at this point how accurate the Chinese data is, but it's not implausible that the kind of heavy-handed quarantining of sick or exposed people which China was engaging in could have kept the spread mostly in Hubei Province and eventually have eradicated the virus even there.
Of course, that phrase "reported cases" is key. China is not a free society, and throughout the crisis the regime has acted to preserve its prestige. It may well be that China is lying to some extent about the number of cases and number of deaths. Even if they aren't intentionally lying, local officials may be hiding the truth from higher officials in order to make themselves look better. And of course, all countries' counts are suspect at this point because information is difficult to come by. There's no way to know at this point how accurate the Chinese data is, but it's not implausible that the kind of heavy-handed quarantining of sick or exposed people which China was engaging in could have kept the spread mostly in Hubei Province and eventually have eradicated the virus even there.
Free societies such as South Korea and Taiwan have successfully crushed their COVID-19 outbreaks through serious but less inhumane methods. These Asian countries in particular had good reason to take an outbreak of a new coronavirus seriously. They had borne the brunt of the SARS outbreak -- a related coronavirus which was much more fatal but much less easily spread -- eighteen years ago, and so they had the experience of having identified, isolated, and eliminated a deadly new respiratory virus.
A recent Twitter thread described what South Korea's measures to contain the virus are like to this day:
Needless to say, lockdowns and quarantines are not without economic cost. China has the advantage of having their initial outbreak behind them, and having taken such extreme measures that their outbreak was comparatively short. Nonetheless, their economy has taken a considerable hit, and it will continue to do so because a good deal of their economy is centered on making things to export to other countries. When those countries are in their turn going through lockdowns and the recessions related to them, they will be buying less stuff from China. And that's before we consider that people in many countries may feel just a little bit peeved with China before all is said and done.
 The article this above chart comes from, which talks about what China looks like as it slowly reopens its economy, is worth reading.
The article this above chart comes from, which talks about what China looks like as it slowly reopens its economy, is worth reading.
Read Part 2 here.
The coronavirus outbreak and the way that it's been dealt with by our country is such a big topic that even though I've been following the story a great deal and trying to understand it, writing comprehensively on the topic seems daunting. And yet, it's trying to fit the entire topic together in some sort of context that seems most needed. Thus, this post will attempt to tackle first how I came to think about the topic the way I do, and then my understanding where we are, how we got here, and where we may be going.
How I Got This Way
I heard about the coronavirus fairly early (mid-January) because the company I work for has offices in China and in Taiwan, and so we had colleagues who were affected by the Chinese lockdown and travel restrictions back in January. I also knew from seeing the dramatic slowdown in sales to our Chinese customers (and from my Chinese colleagues who were working from home despite being over five hundred miles from Wuhan) that China was making a massive effort to contain the virus and that that was likely to have significant economic effects.
And yet, I was blind to the possibility that we would actually end up with a significant outbreak in the US. Looking back, there wasn't any rational basis for this blindness. Rather, there was a sort of habitual interpretive filter that we often apply instead of reason because it's quicker and easier. Various other outbreaks had occurred without becoming widespread in the US (SARS, MERS, Zika, Ebola, etc.) and so I made the assumption that somehow or other -- through luck or the efforts of epidemiologists or travel screening or the blessings of first world life we take for granted -- we wouldn't get more than a smattering of cases in the US.
It was in early March, as it began to become clear this was not the case, that I started to play catch up on reading about the virus. In my reading I was fortunate, in that the first people I looked to were people I knew to be scientifically and statistically literate. I quickly realized that Razib Kahn of the Gene Expression blog was taking the virus very seriously. Razib is someone I've been reading off and on for nearly fifteen years, almost since this blog began. His scientific work is in genetics, he's got a strong understanding of data analysis, and he's also very historically literate. Nor is he easily led by convention. (The NY Times at one point invited him to be a recurring contributor and then pulled the invitation because they decided he was too un-PC.) Another person whose thinking about the virus guided my early impressions was Josiah Neeley who ages ago was the libertarian voice on Vox Nova and wrote the Blackadder blog. Now you can hear him under his own name at the Urbane Cowboys podcast (which is one I try to listen to every week even though I don't like podcasts as a format.) If you want to hear my two main influences come together, Razib was a guest on the Urban Cowboys podcast in this episode back in March focusing on the coronavirus. Through them I found a number of people on twitter who seemed to be addressing the topic realistically and linking to good scientific content.
This was my background when I wrote my first post touching on an aspect of the coronavirus outbreak and the measures proposed to slow it's spread back on March 14th, which not-coincidentally was the day after my last day in the office at my employer, as those of us not working the manufacturing plant had all been told to work from home until further notice. (That I have a job I'm able to do from home and remain gainfully employed is a good fortune for which I am duly grateful, though the economic effects of the pandemic will still be hitting the company hard and thus we're dealing with pay cuts, etc. in order to keep the company solvent.)
But as I was learning about the situation, the situation and the response to it by various countries was changing rapidly. What are we to make of these developments?
Coronavirus: Origin Story
I have no intention of trying to dig into the question of how the virus got loose in the first place, as this is one of the things it will probably take us longest to have clear information about. What does seem pretty clear, however, is that China first went through a phase of trying to pretend the outbreak did not exist. While they're an oppressive autocracy, their instincts here were probably not that different from the instincts that have made more democratic governments deny the seriousness of the situation at first. They didn't want to scare people, admit possible incompetence, and suffer the economic disruption of a major disease outbreak, and so at first they hoped it would go away. It didn't. So China then went into a second phase of trying to actively suppress the disease. To that end, they shut down travel between the city of Wuhan (where the outbreak had originated) and other parts of China. They put people both inside and outside Hubei province under lockdown. And then within Wuhan itself (which is by population about the size of New York City, but is only the 9th most populous city in China) they began to enforce strict quarantines of all sick people and even of people who had been exposed to sick people. China being a repressive and secretive society, it's hard to know for sure what did and didn't happen, but there are rhumors that spread from China at the time about sick people being welded into their apartments and left to die.

Whether these darker stories are true or the CCP was merely pursuing a conventional but strict set of isolation rules, the result was that although by the end of January there had been cases identified in many parts of China as well as in nearby countries and even in the US, the virus never spread widely in Chinese provinces other than Hubei. Pulling down data from the John Hopkins data portal, and charting the number of reported new cases each day, Hubei frequently reported over a thousand new cases a day in late January and early February, while the other provinces with the largest outbreaks were reporting just over a hundred.

Free societies such as South Korea and Taiwan have successfully crushed their COVID-19 outbreaks through serious but less inhumane methods. These Asian countries in particular had good reason to take an outbreak of a new coronavirus seriously. They had borne the brunt of the SARS outbreak -- a related coronavirus which was much more fatal but much less easily spread -- eighteen years ago, and so they had the experience of having identified, isolated, and eliminated a deadly new respiratory virus.
A recent Twitter thread described what South Korea's measures to contain the virus are like to this day:
1) Upon arrival, they take your temperature at the airport and ask if you’ve experienced any symptoms. If you have, they move you to a separate area and give you a coronavirus test. If you haven’t, they take you to another area and interview you. They also install ankle braceletsYou can read the whole thread here.
2) You are required to install an app on your phone and enable location tracking all the time. You are required to self-report symptoms in the app twice a day. If you don’t have symptoms, you need to report that too. This goes on for a period of 14 days
During this time, you are not allowed to leave the quarantine dormitory or your home if you’ve chosen to self-isolate at home. You cannot take public transportation or taxi, and you cannot self-isolate in a hotel or Airbnb. If you don’t have a home, you must use the dorm.
If you break quarantine, you are fined $10,000 USD and face jail time. Also, they check your location on your phone frequently. My wife had her location checked 37 times in a 3 day span. And they’ve caught enterprising folks who leave their phone at home and go out.
During this self-isolation, you cannot have contact with anyone during this time. They give you special trash bags to throw away your trash in, and people in hazmat suits come and collect your trash upon request.
You are assigned to a case worker who is responsible for making sure you are following all the orders. They will call you and text you to make sure you are OK. They also will send you care packages that contains a lot of food, gloves and masks, sanitary pads for women, etc.
3) If there’s a new coronavirus case in your general area (same city or district), you get a Public Safety Alert on your phone that tell you about the person (age, male/female, city) and provides updates as they receive them.
Needless to say, lockdowns and quarantines are not without economic cost. China has the advantage of having their initial outbreak behind them, and having taken such extreme measures that their outbreak was comparatively short. Nonetheless, their economy has taken a considerable hit, and it will continue to do so because a good deal of their economy is centered on making things to export to other countries. When those countries are in their turn going through lockdowns and the recessions related to them, they will be buying less stuff from China. And that's before we consider that people in many countries may feel just a little bit peeved with China before all is said and done.

Read Part 2 here.
Friday, May 08, 2020
The Cincinnatus Option

I was thinking about the kinds of mythology society retells about service.
If we think of the early American republic, one of the key myths was the myth of Cincinnatus. The reason why his story was important to the American founders was that he displayed a powerful consciousness of the division between the individual and the duties of the state. When the Senate came to Cincinnatus as he was plowing his field, they called upon him to leave his life as a private person and save the state from a threat. He left his plow in the field, went to serve the state as dictator (an office which according to the laws of the Roman Republic had complete power for a short period of time) and then as soon as he was done surrendered his power and returned to plowing his field.
Cincinnatus does not see himself as specially anointed or empowered as a person. Rather, he is an ordinary citizen who is asked for a short time (as short at time as possible) to act with extraordinary power to protect the state and his fellow citizens. But his power is not personal. He does not, in and of himself, have the right to wield power. He has power only to the extent it is given to him for a time by the state.
It struck me that in a sense this is the opposite to many of our modern mythologies. There is perhaps no more clear example of a modern mythology than the superheroes that populate so many of our hit movies. And what is the standard story that we see in superhero stories? They have a special set of abilities which they must live up to by serving society. Take, for instance, the central story of basically all the Spiderman movies: He has a special set of abilities which only he has, and thus he must act on behalf of a city that needs him. Spiderman is not an ordinary person briefly called up to act on behalf of society, he is a unique person who must always fulfill a special roll because of his special abilities. He cannot go back to his ordinary life because there is only one Spiderman.
A great many other modern stories similarly involve that one special person who must fulfill a destiny for the good of all. Harry Potter is the only one who can defeat Voldemort and save the world of wizards. Neo is The One who can defeat The Matrix. Even a lot of theoretically non-supernatural stories involve some specially gifted character with "a certain set of skills" who must blaze in to save the world from terrible danger.
In all of these cases, the character is special because of some inherent thing about the character. Perhaps that's very convenient for generating sequels, because when danger looms the only choice is to call back that one character who starred in the previous story. But it also suggests a world in which people hold authority within society not because of an office with which they are temporarily entrusted, but rather because of a unique set of abilities which only that character has. These peculiarly gifted characters stand above the law. Harry Potter must save the wizarding world whether their incompetent government actually wants him to or not. Spiderman must fight crime not because he's been legally entrusted with that duty but because the legal authorities are helpless to stop certain evils without his super-powered intervention.
But in a sense, doesn't this great emphasis on the special individual who has authority to act to protect society because of his specialness promote an vision of society in which people who think themselves exceptional would see themselves as heroes for engaging in vigilante actions? Engaging though these stories of special individuals are, when they are the predominant kind of story that we tell about saving society from danger were are probably creating a vision of society in which people feel entitled to step up and take power into their own hands. And yet, the virtue of Cincinnatus, who assumed power only when he was asked to and gave it back as soon as he was able, is surely a virtue that we would like to see lived out in society by those who actually hold power. Surely what we want is for those who have wielded power on behalf of law and order to see themselves as having gone back to being ordinary citizens at the end of their office -- not see themselves as heroes uniquely set apart by a lonely vocation to protect society due to their own special abilities and experiences.
Thursday, May 07, 2020
Thin Skin
Two days ago Darwin and I were booking it on our daily walk, against the chill and the first drops of rain. I was trotting along, proud of my easy jog, when I caught my toe in an uneven patch of sidewalk, and found the ground rapidly rising to meet me. I had time to think,"I'm going all the way to the ground," but not enough time to make any kind of attempt to save myself. The bluster of the evening meant that no one else was out to witness my downfall, but still, it is an ignominious thing to be sprawled on the concrete.
I got up heavily, with Darwin's help, and we continued on our way, but it was clear that I'd done something nasty to my knees. The palms of my hand were rapidly turning a bruisy purple, and my elbows twinged uncomfortably with the force of the jolt. Indeed, once I gingerly peeled off my leggings at home, they lifted skin and blood from my raw knees.
What a thing it is to be over 40! I haven't skinned my knees since I was a featherweight careening around on my bike or running barefoot down a gravel driveway. In those days once bounced back up and cried a little, then ran inside to have Mom wipe up and put a bandaid on the scrapes. Then it was back outside again, and the injury forgotten. Now I hauled myself stiffly upstairs and applied myself to the task of how one could fix sterile pads over an area too large to be covered by a bandaid, when one had no more surgical tape in the house because one's children had found it at some point.
Well, one doesn't fix them, is the answer. I sat in bed with the untaped pads lightly covering the thick film of antibiotic cream on my open flesh, and gave myself up to the idea that I was down for the night. Darwin brought me coffee; my older daughters shared some chocolate they'd spirited away, and the younger ones came up to gawk at my injuries.
"Just like Jesus," I said, contemplating my skinned knee, but I knew I was being pretentious. Jesus fell under the weight of the cross, already suffering from horrendous injuries; my knee took the brunt of nothing other than 41 years and seven children's worth of avoirdupois. Unlike the lamb led to the slaughter, who opened not his mouth, I found myself hissing last night when I stripped off a bandaid that had been pressed over the worse spot. Gad, that stung! And unlike Jesus, I did not have a robe ripped off a body that was one bleeding open mass.
Indeed, as I type this, a child has just climbed on the couch next to me and rammed a solid knee into my bruised one. And I yelped. To have a thin skin means to be touchy, unnecessarily sensitive, and thick skin is considered a cushion against hurts. I'll agree with the latter, but I have to say that thin skin just plain hurts. The slightest coating of the nerves, taut and inflexible, alive to the least pressure. When I bend my knee too far, the scabs groans in protest; when I straighten it too much, the inelastic skin resists.
My elbows only have the slightest ache, and my palm is browning up nicely, but I have a feeling my knee has further to go. I want to walk again today -- it seems better once I get moving and warmed up, and I need the exercise after a day of immobility. Gotta thicken up that skin the healthy way. If you want to sit on my lap, though, the answer is no.
I got up heavily, with Darwin's help, and we continued on our way, but it was clear that I'd done something nasty to my knees. The palms of my hand were rapidly turning a bruisy purple, and my elbows twinged uncomfortably with the force of the jolt. Indeed, once I gingerly peeled off my leggings at home, they lifted skin and blood from my raw knees.
What a thing it is to be over 40! I haven't skinned my knees since I was a featherweight careening around on my bike or running barefoot down a gravel driveway. In those days once bounced back up and cried a little, then ran inside to have Mom wipe up and put a bandaid on the scrapes. Then it was back outside again, and the injury forgotten. Now I hauled myself stiffly upstairs and applied myself to the task of how one could fix sterile pads over an area too large to be covered by a bandaid, when one had no more surgical tape in the house because one's children had found it at some point.
Well, one doesn't fix them, is the answer. I sat in bed with the untaped pads lightly covering the thick film of antibiotic cream on my open flesh, and gave myself up to the idea that I was down for the night. Darwin brought me coffee; my older daughters shared some chocolate they'd spirited away, and the younger ones came up to gawk at my injuries.
"Just like Jesus," I said, contemplating my skinned knee, but I knew I was being pretentious. Jesus fell under the weight of the cross, already suffering from horrendous injuries; my knee took the brunt of nothing other than 41 years and seven children's worth of avoirdupois. Unlike the lamb led to the slaughter, who opened not his mouth, I found myself hissing last night when I stripped off a bandaid that had been pressed over the worse spot. Gad, that stung! And unlike Jesus, I did not have a robe ripped off a body that was one bleeding open mass.
Indeed, as I type this, a child has just climbed on the couch next to me and rammed a solid knee into my bruised one. And I yelped. To have a thin skin means to be touchy, unnecessarily sensitive, and thick skin is considered a cushion against hurts. I'll agree with the latter, but I have to say that thin skin just plain hurts. The slightest coating of the nerves, taut and inflexible, alive to the least pressure. When I bend my knee too far, the scabs groans in protest; when I straighten it too much, the inelastic skin resists.
My elbows only have the slightest ache, and my palm is browning up nicely, but I have a feeling my knee has further to go. I want to walk again today -- it seems better once I get moving and warmed up, and I need the exercise after a day of immobility. Gotta thicken up that skin the healthy way. If you want to sit on my lap, though, the answer is no.
Sunday, May 03, 2020
What You Can Expect When You're Expecting an 18yo
A friend of mine recently said that she finally weighed what she did 18 years ago, and incidentally, her oldest daughter's 18th birthday was in a few days. I laughed, because I now weigh substantially more than I did 18 years ago, when I too was nine months pregnant. I'd say, "Ah, youth,", but really I don't want to be either 23 or nine months pregnant again, and I'm delighted to have a daughter who is 17 years and 358 days old.
But this put me in mind of a question it's rapidly growing too late to ask: what is it that should be done before a child turns 18? What sort of legal documentation or medical issues ought to be dealt with?
(I don't mean educationally or life-skills. After all, we already wrote the world's most definitive post on What Your 18-Year-Old Needs to Know, when we were only nine years away from 18 and knew damn-all everything and wrote 43 posts a month. 43 posts! We just don't know that much anymore.)
Get a checkup, you'll doubtless say, and go to the dentist. Normally I'd agree, but the dentist cancelled all our appointments, and the doctor isn't doing checkups right now. We're willing to dig up all the documentation for her to get one of those schmancy new Federal ID licenses that airport security will accept as ID, except: can't go to the BMV right now. If there are any records we ought to request, any other appointments we ought to make, any papers we need to sign, I'd be glad to know about them. After all, I still have a week.
But this put me in mind of a question it's rapidly growing too late to ask: what is it that should be done before a child turns 18? What sort of legal documentation or medical issues ought to be dealt with?
(I don't mean educationally or life-skills. After all, we already wrote the world's most definitive post on What Your 18-Year-Old Needs to Know, when we were only nine years away from 18 and knew damn-all everything and wrote 43 posts a month. 43 posts! We just don't know that much anymore.)
Get a checkup, you'll doubtless say, and go to the dentist. Normally I'd agree, but the dentist cancelled all our appointments, and the doctor isn't doing checkups right now. We're willing to dig up all the documentation for her to get one of those schmancy new Federal ID licenses that airport security will accept as ID, except: can't go to the BMV right now. If there are any records we ought to request, any other appointments we ought to make, any papers we need to sign, I'd be glad to know about them. After all, I still have a week.
Saturday, May 02, 2020
Quarantine Theater presents: 12 Angry Men

Places! Click over to arenafair.com at 7pm EST to listen to Darwin as Juror 12 in 12 Angry Men, presented radio-style. And may God have mercy on your souls.